Download
1 / 23
410 likes | 1.54k Views
Lymphangitic Carcinomatosis. A Reinders Department of Radiology UFS. Case Presentation. 52 year old female patient Retroviral disease negative Previously known with right sided breast carcinoma Had right mastectomy and axillary clearance Now clinically showed progression

E N D
LymphangiticCarcinomatosis A Reinders Department of Radiology UFS
Case Presentation • 52 year old female patient • Retroviral disease negative • Previously known with right sided breast carcinoma • Had right mastectomy and axillary clearance • Now clinically showed progression • CXR shows scattered infiltrates • Pleural effusion • Pleural changes on the right
Case presentation • Medical/social history • No significant • Special investigations • Nuclear medicine • Bone Scintigram • “Degenerative lesions in thoracic spine – unable to exclude metastases” • Radiology • CXR • CT Chest/abdomen and pelvis
LymphangiticCarcinomatosis • 6 – 8% of all pulmonary metastases • Tumor cell accumulation within connective tissue1 • Tumor cell embolizationof blood vessels • Subsequent lymphatic obstruction • Interstitial oedema • Collagen deposition • Associated cancers • Cervic/colon • Stomach • Breast • Pancreas • Thyroid • Larynx “Certain cancers spread by plugging the lymphatics”1
Imaging • CXR1 • Reticular/reticulonodularopacities • Coarsenendbronchovascularmarkings • Kerley A and B lines • Small lung volumes • Hilar/mediastinallymphadenopathy • Pleural effusions
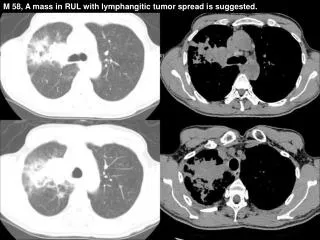
HRCT • Normal lung architecture1 • Focal/diffuse/unilateral/bilateral distribution • Thickenendinterlobular septa • Thickenendcentrilobularbronchovascularbundle • “Dot in box” appearance • Pleural effusions (30 – 50%) • Lymphadenopathy (30 – 50%)
HRCT Pulmonary lymphangiticcarcinomatosis. Available from URL:http://www.radiopedia.org2
Differential diagnoses1 • Pulmonary Tuberculosis • Hypersensitivity pneumoniae • Sarcoidosis • Cardiogenic Pulmonary Edema Thinking cap.....
Pulmonary Tuberculosis • Primary TB3,4 • Consolidation • Lymphadenopathy • Pleural effusion • Regresses • Secondary TB • “Reactivation” • Consolidation apical segments/superior segment lower lobes • Cavitation • Miliary TB • 2 – 3 mm nodules in random distribution throughout lung
Pulmonary Tuberculosis • Clinial history • Immunocompromised • “Tree -in-bud appearance” • Endobronchial spread • Simultaneous occurance with LCM • Rare • May also present with septal thickening • Almost impossible to distinguish radiologically • Incidental findings in immunocompromised patients • Secondary reactivation of Tuberculosis5 Tuon FF, Miyaji KT, DE Vidal PM et al. Simultaneous occurence of pulmonary tuberculosis and carcinomatouslymphangitis. Rev. Oc Bras Med Trop. 2007 Jan-Feb; 40(1) :76-7
Pulmonary Tuberculosis Left: Active pulmonary Tuberculosis with cavitation in the apical segment of right lower lobe Right: Tree in bud appearance indicating endobronchial spread
Hypersensitivity Pneumonia • Extrinsic Allergic Alveolitis • “Farm worker’s lung” • “Bird fancier’s lung” • Stages3 • Acute • Subacute • Ill defined centrilobular nodules • Mosaic pattern • Bronchiolitis with air trapping (lucencies) + patchy areas of infiltration (ground glass) • Chronic • Mosaic pattern • Fibrosis and parenchymal distortion in midzone distribution • Fibrosis typically through whole lung • From periphery to centrum
Hypersensitivity Pneumonia Morissa AM, Nishimurab S, Huanga L. Subacute hypersensitivity pneumonitis in an HIV infected patient receiving antiretroviral therapy. Thorax 2000;55:625-627 doi:10.1136/thorax.55.7.6256
Sarcoidosis • Systemic disorder of unknown origin3,4 • Non caseatinggranulomas in multiple organs • 90% of patients have lung involvement • Lobar predominance • Upper and midzone predominance • Small nodules in perilymphatic distribution • 1-2-3 Sign + calcifications • Silzbach classification • Stage 0 = normal lungs • Stage 1 = Lymphadenopathy only • Stage 2 = Lung involvement and lymphadenopathy • Stage 3 = Lung involvement only • Stage 4 = Fibrosis
Sarcoidosis Pulmonary sarcoidosis. Available from URL: http://www.radiopedia.org2
Cardiogenic Pulmonary Edema • HRCT3 • Bilateral smooth septal thickening • Ground glass opacity • Perihilar and gravitational distribution of fluid • Cardiomegaly • Pleural effusion
Cardiogenic Pulmonary Edema Smithuis R, Van Delden O, Schaefer-Prokop C. HRCT part II: Key findings in Interstitial Lung Diseases.3 Available from URL: http://www.radiologyassistant.nl/en/
Bibliography • 1. Chest Disorder. In: Dahnert W. Editor. Radiology Review Manual. 6th Edition. Lippincot Williams & Wilkins. 2007; p509 • 2. Images available from URL: http://www.radiopedia.org • 3. Smithuis R, Van Delden O, Schaefer-Prokop C. HRCT part II: Key findings in Interstitial Lung Diseases. Available from URL: http://www.radiologyassistant.nl/en/ • 4. Chest Imaging. In: Weissleder R, Wittenberg J, Harisinghani MG, Chen JW. Editors. Primer of Diagnostic Imaging. 4th Edition. Mosby Elsevier 2007; p34 - 35 • 5. Tuon FF, Miyaji KT, de Vidal PM et al. Simultaneous occurence of pulmonary tuberculosis and carcinomatouslymphangitis. Rev. Oc Bras Med Trop. 2007 Jan-Feb; 40(1) :76-7 • 6. Morissa AM, Nishimurab S, Huanga L. Subacute hypersensitivity pneumonitis in an HIV infected patient receiving antiretroviral therapy. Thorax 2000;55:625-627 doi:10.1136/thorax.55.7.625