Download
1 / 22
240 likes | 685 Views
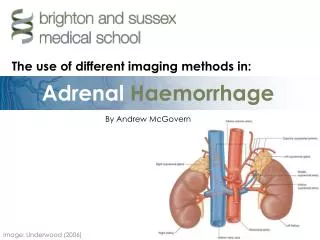
ADRENAL EXCESS DISORDER. Overview of Adrenal Gland. Adrenal cortex – outer shell Mineralocorticoids – Aldosterone Glucocorticoids – Cortisol Secondary sex hormones – Androgens and estrogens Adrenal medulla – inner core works as part of the sympathetic nervous system

E N D
Overview of Adrenal Gland • Adrenal cortex – outer shell • Mineralocorticoids – Aldosterone • Glucocorticoids – Cortisol • Secondary sex hormones – Androgens and estrogens • Adrenal medulla – inner core • works as part of the sympathetic nervous system • Produces epinephrine and norepinephrine
Cushing’s disease & Cushing’s syndrome • Risk Factors: • Endogenous (Cushing’s disease) • Adrenal hyperplasia • Adrenocortical carcinoma • Carcinoma of the lungs, GI tract, or pancreas, pituitary carcinoma • Exogenous (Cushing’s syndrome) • Organ transplant • Chemotherapy • Autoimmune diseases • Asthma • Allergies • Chronic inflammation diseases Cushing’s Disease (endogenous) • increased secretion of cortisol caused by increased amounts of ACTH secreted by pituitary gland. Cushing’s syndrome (exogenous) • resulting from chronic and excessive production of cortisol by adrenal cortex or administration of large doses
Signs and Symptoms: • Moon face • Buffalo hump • Truncal obesity • Weakness • Fatigue • Back and joint pain • Irritability or depression • Thin, fragile skin • Bruising and petechiae • Hypertension • Tachycardia • Weight gain • Dependent edema
Diagnostics: • H&P exam • Mental status exam • Plasma cortisol levels, • Plasma ACTH level • CBC, WBC, • Blood chemistries for sodium, potassium, glucose • Dexamethasone suppression test • 24-hr urine for free cortisol • CT scan, MRI. • Collaborative care: • Decrease sodium intake, increase intake of potassium, protein, calcium • Monitor intake output, daily weight • Assess signs of hypervolemia • Skin care, protect against skin breakdown and infection • Medications: Aminoglutethimide (Cytadren), ketoconazole (Nizoral) • Chemotherapy • Hypophysectomy – removal of pituitary gland • Adrenalectomy – removal of the adrenal gland
Addison’s Disease • Adrenocortical insufficiency caused by damage of the adrenal cortex • Decreased aldosterone and cortisol • Adrenal crisis (medical emergency) – acute adrenal insufficiency, caused by sepsis, trauma, stress, adrenal hemorrhage, steroid withdrawal • Risk Factors: • Primary - autoimmune dysfunction, TB, hystoplasmosis, adrenalectomy, cancer • Secondary – steroid withdrawal, hypophysectomy, pituitary neoplasm • Signs and Symptoms: • Hyperpigmention • Weakness and fatigue • Nausea and vomiting • Dizziness with orthostatic hypothension • Severe hypotension • Dehydration • Hyperkalemia • Hypglycemia • hypercalcemia (ATI Nursing Education)
Diagnostics: • H&P exam • Plasma cortisol level • Urine cortisol and aldosterone levels • Serum electrolytes • ACTH-stimulate test • CT scan, MRI • ECG, XRAY, CT http://www.youtube.com/watch?v=qfC2te9Unbw • CollaborativeCare: • Monitor fluid deficits • Administer prescribed hydrocortisone, continuous infusion of boluses • Treat hypercalemia • Treat Hypoglycemia • Medications : • hydrocortisone (Cortef), Prednisode, cortisone • Fludrocortisone (Florinef)
Hyperaldosteronism • Characterized by excessive aldosterone secretion. • Hallmark disease – hypertension with hypokalemic alkalosis. • Primary hyperaldosteronism (PA) – caused by small solitary adrenocortical adenoma. • Secondary hyperaldosteronism– occurs in response to a nonaderenal cause and elevated aldosterone levels such as renal artery. • Risk factors : • Age 30 -50 y.o. • renal artery stenosis • renin-secreting tumors • Chronic kidney disease
Signs and symptoms: • Hypernatremia • Hypertension • Headache • Muscle weakness, Fatigue • Cardiac dysrhythmias • Glucose intolerance • Metabolic alkalosis • Tetany • Diagnostic: • CT , MRI • 18 hydroxycorticosterone- (50ng/dL) Treatment: • Adrenalectomy – 80% control HTN • Potassium • Calcium channel blocker • Potassium sparing diuretic (cytaren) • dexamethasone
Pheochromocytoma • A tumor of the center of the adrenal gland and medulla • Excessive catecholamines (epinephrine, norepinephrine • 10% - malignant • Severe hypertension Risk factors: • Neurofibromatosis • Multiple endocrine neoplasia syndrome • Age 40 – 60 y,o • Signs and symptoms: • Pain in chest/abdominal • Hypertension • Headaches • Diaphoresis • Palpitations • Heat intolerance • Tremors • Apprehension
Laboratory test: • Vanillymandelic acid (VMA) testing – 24 hr. urine collection • VMA normal level 2 to 7 mg/24hr. Diagnostic procedures: • Clonidine suppression test • Administration of phenotolamine (Regitine) • Treatments: • Alpha adrenergic blockers – prazosin, phenoxybenzmine • Beta blockers – metoprolol (Lopressor) • Glucocorticoids – Prednisone (Deltasone) • Adrenalectomy surgery – complications of hypertensive crisis
NCLEX QUESTION #1 • A client is diagnosed with pheochromocytoma. A nurse prepares a plan of care for the client; while planning, the nurse understand that pheochromocytoma is a condition that: • 1. causes profound hypotension • 2. is manifested by severe hypoglycemia • 3. is not curable and is treated symptomatically • 4. causes the release of excessive amounts of catecholamines
Answer: 4 • Rationale: Pheochromocytoma is a catecholamine-producing tumor and causes secretion of excessive amounts of epinephrine and norepinephrine. Hypertension is the principal manifestation, and the client has episodes of high blood pressure accompanied by pounding headaches. The excessive release of catecholamine also results in excessive conversion of glycogen into glucose in the liver.
NCLEX QUESTION #2 • A nurse is providing discharge instructions to a client who has Cushing’s syndrome. Which client statement indicates that instructions related to the dietary management are understood? • 1. “I can eat food that have a lot of potassium in them.” • 2. “I will need to limit the amount of protein in my diet.” • 3. “I am fortunate that I can eat all the salty foods I enjoy.” • 4. “I am fortunate that I do not need to follow any special diet.”
Answer: 1 Rationale: A diet low in carbohydrates and sodium but ample in protein and potassium is encouraged for a client with Cushing’s syndrome. Such diet promotes weight loss, reduction of edema and hypertension, control of hypokalemia, and rebuilding of wasted tissue.
NCLEX QUESTION #3 • A nursing instructor asks a student to be describe the pathophysiology that occurs in Cushing’s disease. Which statement by the student indicates and accurate understanding of this disorder? • 1. “Cushing’s disease results from an oversecretion of corticotropic hormones.: • 2. “Cushing’s disease results from an undersecretion of mineralocorticoid hormones.” • 3. “Cushing’s disease results from an undersecretion of mineralocorticoid hormones.” • 4. “Cushing disease results from an increased pituitary secretion of adrenocorticotropic hormone.”
Answer: 4 • Rationale: Cushing’s disease is a metabolic disorder characterized by abnormally increased secretion (endogenous) of cortisol, caused by increased amounts of adrenocorticotropic hormone (ACTH) secreted by the pituitary gland. Addison’s disease is hypo secretion of adrenal cortex hormones from the adrenal gland.
NCLEX QUESTION #4 • A nurse is caring for a client with pheochromocytoma who is scheduled for adrenalectomy. IN the preoperative period, the priority nursing action would be to monitor: • 1. Vital signs • 2. Intake and output • 3. Blood urea nitrogen results • 4. Urine for glucose and ketones
Answer: 4 • Rationale: Pheochromocytoma is a catecholamine-producing tumor and causes secretion of excessive amounts of epinephrine and norepinephrine. Hypertension is the principal manifestation, and the client has episodes of high blood pressure accompanied by pounding headaches.
NCLEX QUESTION #5 • A nurse is performing an assessment on a client with pheochromocytoma. Which of the following assessment data would indicate a potential complication associated with this disorder? • 1. A coagulation time of 5 minutes • 2. A urinary output of 50 mil per hour • 3. A blood urea nitrogen level of 20 mg/dL • 4. A heart rate that is 90 beats/min and irregular
Answer: 4 • Rationale: the complications associated with pheochromocytoma include hypertensive retinopathy, myocarditis, increased platelet aggregation, and stroke. Death can occur from shock, stroke, renal failure, dysrhythmias or dissection aortic aneurysm.
References • Lewis, S. L., Dirksen, S. R., Heitkemper, M. M., Bucher, L., & Camera, I. M. (2011). Medical-surgical nursing, assessment and management of clinical problems. (8th ed., Vol. 2, pp1430-1433 &1276-1284). St. Louis, MO: Mosby Inc. • RN Adult Medical Surgical Nursing Review Module Edition 8.0 pages 1066-1091 • Silvestri, L. A., (2012). Saunders Q&A review for the NCLEX-RN examination. (5th ed.)St. Louis, MO: Elsevier Inc. • Vicennati, V., Repaci, A., di Dalmazi, G., Rinaldi, E., Golfieri, R., Giampalma, E., & ... Pasquali, R. (2012). Combined Aldosterone and Cortisol Secretion by Adrenal Incidentaloma. International Journal Of Surgical Pathology, 20(3), 316-319. doi:10.1177/1066896911427036 • Terzolo, M. M., Pia, A. A., & Reimondo, G. G. (2012). Subclinical Cushing's syndrome: definition and management. Clinical Endocrinology, 76(1), 12-18. doi:10.1111/j.1365-2265.2011.04253.x • http://www.youtube.com/watch?v=qfC2te9Unbw