Download
1 / 76
760 likes | 796 Views
This article explores the structure and function of bones, ligaments, muscles, and tendons, as well as the processes of inflammation and healing. It also discusses the clinical implications for athletes and rehabilitation.

E N D
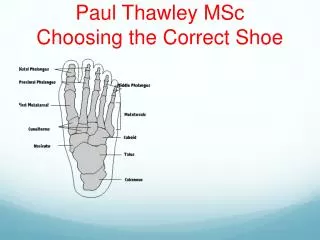
Anatomy and Physiology of Bone, Ligament, Muscle and tendon.Physiology of injury and tissue repairThe inflammatory response and healing Clinical considerations Paul Thawley MSc
Learning objectives • Formulate a clear understanding of the structure and form of bone, ligament and muscle on a molecular and macro level. • Be able to demonstrate the relative reparative mechanisms • Understand the implications for the athlete and clinical rehabilitation.
Musculoskeletal system Give the body its structural form – specialised connective tissues Protect vital organs Promotes efficient movement despite forces of gravity Store salts and other substances needed for metabolism Produce red blood cells
Musculoskeletal system - joints • Where bones interact • Synarthrosis – a joint that does not permit movement, Skull in adults • Diarthrosis (synovial joints) • Monoaxial: hinge or pivot joints • Biaxial: gliding, sliding or saddle joints • Triaxial: ball and socket joints • Ligaments • Joint capsule –synovial fluid
Bone structure Diaphysis Epiphysis Medullary canal Periosteum Cartilage
Types of Bone • Lamellar Bone • Collagen fibers arranged in parallel layers • Normal adult bone • Woven Bone (non-lamellar) • Randomly oriented collagen fibers • In adults, seen at sites of fracture healing, tendon or ligament attachment and in pathological conditions
Bone Composition • Cells • Osteocytes • Osteoblasts • Osteoclasts • Extracellular Matrix • Organic (35%) • Collagen (type I) 90% • Osteocalcin, osteonectin, proteoglycans, glycosaminoglycans, lipids (ground substance) • Inorganic (65%) • Primarily hydroxyapatite Ca5(PO4)3(OH)2
Lamellar Bone • Cortical bone • Comprised of osteons (Haversian systems) • Osteons communicate with medullary cavity by Volkmann’s canals
Lamellar Bone • Cancellous bone (trabecular or spongy bone) • Bony struts (trabeculae) that are oriented in direction of the greatest stress
Woven Bone • Coarse with random orientation • Weaker than lamellar bone • Normally remodeled to lamellar bone Figure from Rockwood and Green’s: Fractures in Adults, 4th ed
Osteoblasts • Derived from mesenchymal stem cells • Line the surface of the bone and produce osteoid • Immediate precursor is fibroblast-like preosteoblasts Picture courtesy Gwen Childs, PhD.
Osteocytes • Osteoblasts surrounded by bone matrix • trapped in lacunae • Function poorly understood • regulating bone metabolism in response to stress and strain Picture courtesy Gwen Childs, PhD.
Components of Bone Formation • Cortex • Periosteum • Bone marrow • Soft tissue
Prerequisites for Bone Healing • Adequate blood supply • Adequate mechanical stability
Mechanisms of Bone Formation • Cutting Cones • Intramembranous Bone Formation • Endochondral Bone Formation
Cutting Cones • Primarily a mechanism to remodel bone • Osteoclasts at the front of the cutting cone remove bone • Trailing osteoblasts lay down new bone Courtesy Drs. Charles Schwab and Bruce Martin
Intramembranous (Periosteal) Bone Formation • Mechanism by which a long bone grows in width • Osteoblasts differentiate directly from preosteoblasts and lay down seams of osteoid • Does NOT involve cartilage
Endochondral Bone Formation • Mechanism by which a long bone grows in length • Osteoblasts line a cartilage precursor • The chondrocytes hypertrophy, degenerate and calcify (area of low oxygen tension) • Vascular invasion of the cartilage occurs followed by ossification (increasing oxygen tension)
Blood Supply • Long bones have three blood supplies • Nutrient artery (intramedullary) • Periosteal vessels • Metaphyseal vessels Periosteal vessels Nutrient artery Metaphyseal vessels Figure adapted from Rockwood and Green, 5th Ed
Vascular Response in Fracture Repair • Fracture stimulates the release of growth factors that promote angiogenesis and vasodilation • Blood flow is increased substantially to the fracture site • Peaks at two weeks after fracture
Mechanical Stability • Early stability promotes revascularization • After first month, loading and interfragmentary motion promotes greater callus formation
Mechanical Stability • Mechanical load and small displacements at the fracture site stimulate healing • Inadequate stabilization may result in excessive deformation at the fracture site interrupting tissue differentiation to bone (soft callus) • Over-stabilization, however, reduces periosteal bone formation (hard callus)
Stages of Fracture Healing • Inflammation • Repair • Remodeling
Inflammation • Tissue disruption results in hematoma at the fracture site • Local vessels thrombose causing bony necrosis at the edges of the fracture • Increased capillary permeability results in a local inflammatory milieu • Osteoinductive growth factors stimulate the proliferation and differentiation of mesenchymal stem cells
Repair • Periosteal callus forms along the periphery of the fracture site • Intramembranous ossification • initiated by preosteoblasts • Intramedullary callus forms in the center of the fracture site • Endochondral ossification at the site of the fracture hematoma • Chemical and mechanical factors stimulate callus formation and mineralization
Repair Figure from Brighton, et al, JBJS-A, 1991.
Remodeling • Woven bone is gradually converted to lamellar bone • Medullary cavity is reconstituted • Bone is restructured in response to stress and strain (Wolff’s Law)
Mechanisms for Bone Healing • Direct (primary) bone healing • Indirect (secondary) bone healing
Direct Bone Healing • Mechanism of bone healing seen when there is no motion at the fracture site (i.e. rigid internal fixation) • Does not involve formation of fracture callus • Osteoblasts originate from endothelial and perivascular cells
Direct Bone Healing • A cutting cone is formed that crosses the fracture site • Osteoblasts lay down lamellar bone behind the osteoclasts forming a secondary osteon • Gradually the fracture is healed by the formation of numerous secondary osteons • A slow process – months to years
Components of Direct Bone Healing • Contact Healing • Direct contact between the fracture ends allows healing to be with lamellar bone immediately • Gap Healing • Gaps less than 200-500 microns are primarily filled with woven bone that is subsequently remodeled into lamellar bone • Larger gaps are healed by indirect bone healing (partially filled with fibrous tissue that undergoes secondary ossification)
Direct Bone Healing Figure from http://www.vetmed.ufl.edu/sacs/notes
Indirect Bone Healing • Mechanism for healing in fractures that are not rigidly fixed. • Bridging periosteal (soft) callus and medullary (hard) callus re-establish structural continuity • Callus subsequently undergoes endochondral ossification • Process fairly rapid - weeks
Local Regulation of Bone Healing • Growth factors • Cytokines • Prostaglandins/Leukotriens • Hormones • Growth factor antagonists
Stress fracture Partial or incomplete fracture of the bone that occurs when repeated rhythmic submaximal loads are applied to the bone Failure or a crack in the bone Difficult to spot on x-rays – bone scan/MRI Treatment: protect from stresses/unload bone Prevention strategies
Implications for rehabilitation following bone injury • What are they? • full repair • Previous injury mechanism stress related • Prolonged immobilisation • conditioning • Joint restriction altered biomechanics • MM imbalance and risk of secondary injury • Psych effects
Ligament function Connect bone with bone Augment the static mechanical stability of joints Prevent excessive or abnormal motion Sensory source – protective and propioceptive feedback; neuromuscular dynamic control of stability
Ligament composition Cells (fibroblasts) 20%, and ECM (collagen) 80% 90% of collagen is type 1 (10% type 3) Crosslinking and quarter-staggered array Less parallel arrangement of collagen fibrils in ligaments - can resist forces in many directions
Ligament & tendon insertion • 4 zones of indirect insertion • Perforating fibres of Sharpey cross all 4 zones • Gradual change in structural properties results in increased stiffness and decreased stress concentration minimising injury at insertion sites • Ligament fibres insert oblique or orthogonal • Musculotendinous junction – aponeurosis • Blood supply is poor in both • Ligament: insertion sites • Tendon: paratenon, vincula
Grading of strains • I - Spasm or cramp, stiff & sore, rapid recovery without loss of muscle strength, managed conservatively. • USS - normal or focal/ generalalized area of hyperechogenicity with or without perifascial fluid • MRI - oedema/hemorrhage/both with normal muscle morphology • II - Overuse, resolve with rest, include intrasubstance tear and partial detachment of muscle from adjacent fascia or aponeurosis. Present with pain and loss of function. • USS - discontinuity of muscle fibers in echogenic perimysial striae, hypervascular, intramuscular fluid. • MRI - oedema/hemorrhage with tear and disruption up to 50% • III - Complete myotendinous or tendo-osseous tear with avulsion/retraction. Due to violent contraction against firm resistance. Early surgery may be required • USS - complete discontinuity of muscle fibers, associated hematoma. • MRI - complete tear with retraction
Ligament & Tendon healing • Phase 1: inflammatory/haemorrhagic • Haematoma – inflammatory response • Cytokine mediated PMN’s, fibroblast and macrophage migration • Hours to a few days • Phase 2: proliferative • New blood vessels • Fibroblasts produce new matrix - collagen 3 • Weeks • Phase 3: remodelling • Maturation and conversion of collagen 3 to 1 • Alignment of fibres • Max strength at 6 months
Myotendinous junction Shorter sarcomere lengths More organelles/cell More synthetic ability Interdigitation of cell membrane High degree of membrane folding VERY STRONG!
Muscle repair In complete tear, distal portion degenerates rapidly Nerve supply needed for regeneration More proximal injuries have a worse prognosis because of greater muscle bulk denervation Laceration results in scar formation. Myotubes regenerate across the scar Partial lacerations have better prognosis Conplete laceration in muscle belly can recover approx. 50% of previous force generated by muscle Surprisingly, not studied greatly and more work needed