Download
1 / 34
340 likes | 526 Views
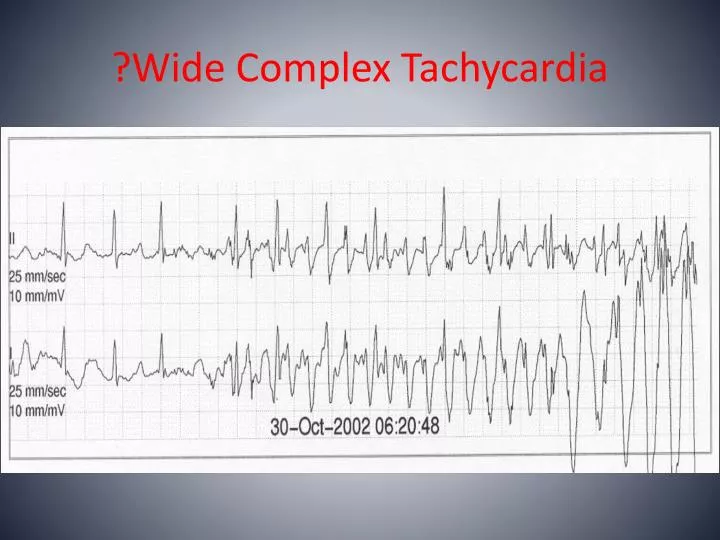
?Wide Complex Tachycardia. Scenario #4. 51 Year Old Male. Presents with 3 hours of chest/epigastric pain, nausea . PMHx: GERD, Borderline HTN, 2 PPD smoker. To ED. Initial ECG. Right Sided Chest Leads. ST Evolution. Treatment. Aspirin, Clopidogrel, Nitrate, O2, ?BB, Statin.

E N D
Scenario #4 • 51 Year Old Male. • Presents with 3 hours of chest/epigastric pain, nausea . • PMHx: GERD, Borderline HTN, 2 PPD smoker. • To ED.
Treatment • Aspirin, Clopidogrel, Nitrate, O2, ?BB, Statin. • Heparin +/- 2b/3A. • Emergent Cath vs. lytics • 100% Occlusion of Large Cx Marginal Branch. • Stented.
Scenario #5 • 84 Year Old Male • Presents to PCP for fatigue. • PMHx: HTN, PAD. • Occasionally “dizzy.” • Fall for unexplained reason last week.
Complete Heart Block • No atrial impulses reach the ventricle. • Thus, leads to escape rhythms. • Junctional or ventricular (Narrow vs. wide). • AV Node supplied by RCA in 90% of people. • Etiology: Increased vagal tone, fibrosis, ischemia, infiltrative disease, myocarditis, SBE, Myotonic MD, hyperkalemia, rate slowing drugs, ablations, alcohol septal ablations.
Complete Heart Block • CHB is a Class 1 recommendation for a PPM irregardless of symptoms in the absence of a STEMI • Other Class 1 Recommendations: Advanced second degree AV Block, Mobitz 1 or 2 with symptoms, Mobitz 2 with wide QRS or chronic bifascicular block, exercise induced second or third degree AV Block in the absence of ischemia.
Treatment of CHB • Correct reversible causes. • Atropine 0.5mg IV (Max 3mg). • Transcutaneous pacing. • Epinephrine/Dopamine drips. • Consider Glucagon if BB Overdose. • Transvenous Pacing. • Permanent Pacemaker.
Scenario #6 • 68 YO Male • PAF 2006 • Recurrence 7/2010- Converted spontaneously after IV Diltiazem and BB. • Jan 2011 Awoken from sleep. “Flip Flopping” • Abn Nuke: distal IL ischemia. • PMHx: HTN, dyslipidemia.
ED Management • IV Diltiazem 25 mg bolus and 10 mg/hr gtt. • BP drops to the 80’s sys • IVF and stop drip • BP rebounds and drip restarted without bolus. • BP drops 80’s systolic. • Why hypotensive?
Why hypotensive? • ?Dry • ?PE • ?Coronary ischemia • ?Tamponade • ?Sepsis • ?Aortic Stenosis • ?Mitral Stenosis
Solution • Took Metoprolol ER 150, Valsartan 320, Amlodipine 10. • 2 Liters of IVF • Calcium Gluconate • Resume IV Cardizem. • ?Why not use Dig? • ?Any argument for CV?
Management • PRECIPITANTS!!! (When did it occur?) • CHADS2=1 (HTN) • ?Heparin/Enoxaparin • ?Warfarin/Dabigatran • ?Cardioversion ? Need for TEE prior. • ?AntiArrhythmic • ?Ablation
CHADS2 Score • CHF 1 point • Hypertension 1 point • Age > 75 1 point • DM 1 point • Stroke/TIA/EP 2 points
Scenario #7 • 30 YO Male. • Presents with sharp, pleuritic chest pain. • URI symptoms 3 weeks ago. • Normal vitals. No fever. • Mild leukocytosis, negative trop. Other labs WNL. • Found leaning over his tray table in the ED. • CXR unremarkable. • “Funny” sound heard on heart auscultation. • Called for ? STEMI although doubted by ED staff secondary to age.
Acute Pericarditis-ECG Changes • Stage 1 = Diffuse ST Elevation/PR Depression. • Stage 2 = Normalization of above changes. • Stage 3 = Diffuse T wave Inversion. • Stage 4 = Normalization of T waves. • Why are changes diffuse? • How do you differentiate from a STEMI? • What does ECHO show? Exam?
Acute Pericarditis - Etiologies • Inflammatory/Autoimmune • Drugs • Metabolic • Trauma • Cardiac • Radiation • Malignancy • Infectious • idiopathic
Pericarditis - Treatment • Treat underlying cause. • Nsaid/Aspirin. • Colchicine. • Steroids. • Pericardiocentesis. • Pericardial Window.