Download
1 / 20
230 likes | 673 Views
FIBRINOLYTIC DRUGS VIJAYA LECHIMI RAJ. Learning Outcomes. On completing this lecture, you should be able to: Classify the fibrinolytic drugs Discuss the mechanism of action of fibrinolytic drugs e.g streptokinase, alteplase Discuss briefly the pharmacology of streptokinase and alteplase

E N D
FIBRINOLYTIC DRUGS VIJAYA LECHIMI RAJ
Learning Outcomes On completing this lecture, you should be able to: • Classify the fibrinolytic drugs • Discuss the mechanism of action of fibrinolytic drugs e.g streptokinase, alteplase • Discuss briefly the pharmacology of streptokinase and alteplase Contents: • Classification of fibrinolytic drugs • Pharmacology of streptokinase and alteplase
Introduction • Acute thromboembolic disease maybe treated by administration of agents that activate the conversion of plasminogen to plasmin • Plasmin is a serine protease that hydrolyses fibrin and thus dissolves clots
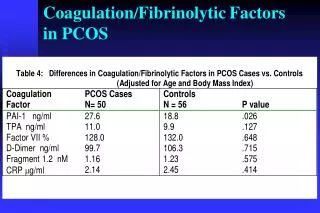
Streptokinase – first to be approved • Causes systemic fibrinolytic state that can lead to bleeding problems • Alteplase – acts more locally on the thrombotic fibrin to produce fibrinolysis <fig> • Nearly equal efficacy between streptokinase and alteplase • Thrombolytic therapy is unsuccessful in 20% of infarcted arteries and 15% will close again later • In MI: • When angioplasty is not an option • Until pt can be taken to facility that performs percutaneous coronary interventions • May lyse both normal and pathologic thrombi<next>
Common Characteristics • Mechanism of action: • All act directly or indirectly to convert plasminogen to plasmin cleaves fibrin lyses thrombi • Clot dissolution and reperfusion occur with higher frequency when therapy is initiated early after clot formation • Clots become more resistant to lysis as they age • Increased local thrombi may occur as clot dissolves Enhanced platelet aggregability and thrombosis • Strategy: • Include administration of antiplatelet drugs (aspirin) or antithrombotics (heparin)
Common Characteristics • Therapeutic uses: • Originally for deep vein thrombosis (DVT), serious pulmonary embolism - Now less frequently • Tendency to cause bleeding has blunted their use in acute MI or peripheral arterial thrombosis • Helpful in restoring catheter and shunt function • By lysing clots that cause occlusions • Also used to dissolve clots that result in strokes • Pharmacokinetics: • Usually administered IV • Rapid • Inexpensive • Does not have risks of catheterization
Common Characteristics • Adverse effects: • Do not distinguish between fibrin of unwanted thrombus and of a beneficial hemostatic plug • Hemorrhage is a major side effect • E.g. a peptic ulcer may hemorrhage after injection of a thrombolytic agent<diag> • C/I in pts with healing wounds, pregnancy, history of cerebrovascular accident, metastatic cancer • presence of thrombogenic stimuli may cause rethrombosis after lysis of the initial clot<next>
Alteplase • Formerly known as tissue plasminogen activator (tPA) • Is a serine protease originally derived from human melanoma cells • Now – product of recombinant DNA technology Mechanism of action: • Low affinity for free plasminogen but rapidly activates plasminogen bound to fibrin in a thrombus or hemostatic plug • Fibrin selective and at low doses lyses only fibrin • Contrasts with streptokinase • Acts on free plasminogen • Induces a general fibrinolytic state
Alteplase • Therapeutic uses: • Approved for treatment of myocardial infarction, massive pulmonary embolism and acute ischemic stroke • Superior to streptokinase in dissolving older clots • Administered within 3 hours of onset of ischemic stroke can significantly improve clinical outcome
Alteplase • Pharmacokinetics: • Very short half-life – about 5 mins • Usually 10% of total dose is injected IV as a bolus and remaining drug is administered over 60 minutes • Adverse effects • Bleeding complications including GI and cerebral hemorrhages may occur
Streptokinase • An extracellular protein purified from culture broths of Group C β-hemolytic streptococci • Mechanism of action: • No enzymic activity • Forms an active one-to-one complex with plasminogen • Converts uncomplexedplasminogen to the active enzyme plasmin
Streptokinase • In addition to the hydrolysis of fibrin plugs, the complex also catalyses the degradation of fibrinogen as well as clotting Factors V and VII
Streptokinase • Therapeutic uses: • Acute pulmonary embolism, deep vein thrombosis, acute myocardial infarction, arterial thrombosis and occluded access shunt • Pharmacokinetics: • Is instituted within 4 hours of a MI and is infused for 1 hour • Half-life is less than half an hour • Thromboplastin time is monitored and maintained at 2-5 fold the control value • On discontinuation of treatment, either heparin or oral anticoagulants may be administered
Streptokinase • Adverse effects: • Bleeding disorders • Activation of circulating plasminogen leads to elevated levels of plasmin • May precipitated bleeding by dissolving hemostatic plugs<fig> • In the rare instance of life-threatening hemorrhage, aminocaproic acid may be administered
Streptokinase • Adverse effects: • Hypersensitivity • Streptokinase is a foreign protein and is antigenic • Rashes, fever and rarely, anaphylaxis occur • Circulating antibodies against streptokinase are likely to be present in most patients
Streptokinase • These antibodies can combine with streptokinase and neutralize its fibrinolytic properties • Sufficient quantities must be administered to overwhelm the antibodies and provide a therapeutic concentration of plasmin • Fever, allergic reaction and therapeutic failure may be associated with the presence of antistreptococcal antibodies • Incidence of allergic reactions – 3%