Download
1 / 64
800 likes | 1.54k Views
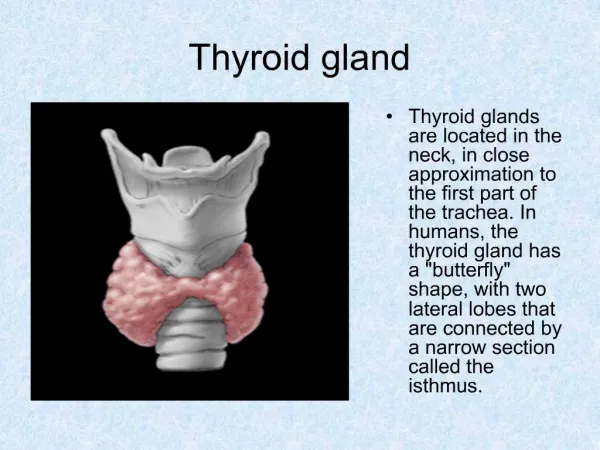
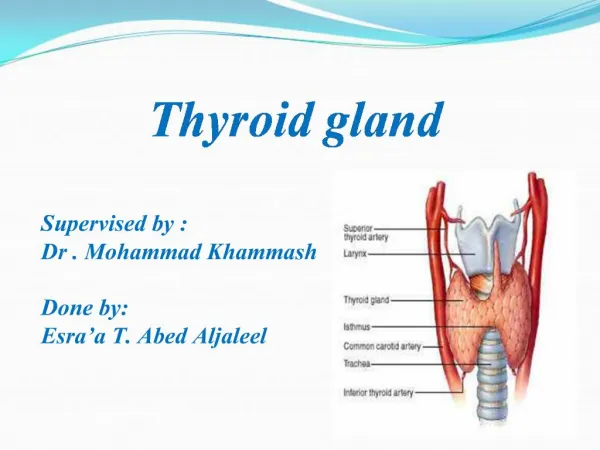
Thyroid gland . Thyroid gland. Largest gland in the body Location : in the neck inferior the larynx and spanning over the ventral surface of trachea Function: Secretion of thyroxin and triiodothyronine Secretion of calcitonin. Thyroid Gland: Hormones and Iodine Metabolism.

E N D
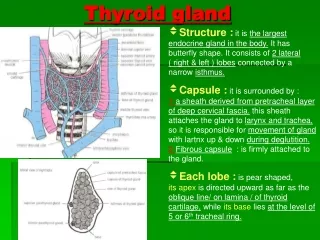
Thyroid gland • Largest gland in the body • Location : in the neck inferior the larynx and spanning over the ventral surface of trachea • Function: • Secretion of thyroxin and triiodothyronine • Secretion of calcitonin
Synthesis of thyroid hormones • Iodide trapping • By sodium iodide symporter • Blocked by: • Thiocyanate SCN- • Perchlorate ClO4- • Pertechnetate TcO4- • Oxidation of iodide • By thyroid peroxidase • Inhibited by: • large intake of iodide >150mcg\day • Thioamides(refer to hyperthyroidism therapy)
Synthesis of thyroid hormones 3. Organification • Tyrosine residues of thyroglobulin is iodinated • Produce monoiodotyrosine residues MDI and diiodotyrosine residues DIT • Inhibited by large intake of iodide >150mcg\day • Thioamides(refer to hyperthyroidism therapy)
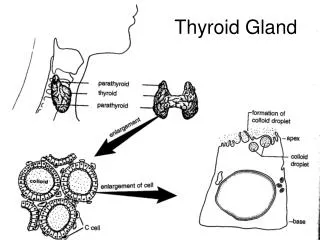
Thyroxine and its precursors: Structure & Synthesis Figure 1-1: Thyroid hormones are made from tyrosine and iodine
Synthesis of thyroid hormones 4. Coupling • DIT+MIT=T3 • DIT+MIT=T4 • Storage : • Along with thyroglobulin 6. Exocytosis and proteolysis • Release of T4 & T3 7. Conversion of T4 to T3 in peripheral tissue
Drugs that inhibit 5’deiodenase • Steroids • Amiodarone • Beta blockers • Thioamides
T4 vs T3 T4 T3 Thyroid gland synthesize 9% 0.4% fr active • Thyroid gland synthesize 90% • 0.04%free • Not active • Long T1\2
Thyroid Hormone Actions Which Increase Oxygen Consumption • Increase mitochondrial Size,Number and Key Enzymes • Increase Plasma membrane Na-K ATPase Activity • Increase Futile Thermogenic Energy Cycles • Decrease Superoxide Dimutase Activity
Effects Of Thyroid Hormones On The Cardiovascular System • Increase heart rate • Increase force of cardiac contractions • Increase stroke volume • Increase Cardiac output • Up-regulate catecholamine receptors
Effects Of Thyroid Hormones On The Respiratory System • Increase resting respiratory rate • Increase minute ventilation • Increase ventilatory response to hypercapnia and hypoxia
Effects Of The Thyroid Hormones On The Renal System • Increase blood flow • Increase glomerular filtration rate
Effects Of The Thyroid Hormones On Oxygen Carrying Capacity • Increase RBC mass • Increase oxygen dissociation from hemoglobin
Effects Of The Thyroid Hormones On Intermediary Metabolism • Increase glucose absorption from the GI tract • Increase carbohydrate,lipid and protein turnover • Down-regulate insulin receptors • Increase substrate availability
Effects Of The Thyroid Hormones In Growth And Tissue Development • Increase growth and maturation of bone • Increase tooth development and eruption • Increase growth and maturation of epidermis,hair follicles and nails • Increase rate and force of skeletal muscle contraction • Inhibits synthesis and increases degradation of mucopolysaccharides in subcutaneous tissue
Effects Of The Thyroid Hormones On The Nervous System • Critical for normal CNS neuronal development • Enhances wakefulness and alertness • Enhances memory and learning capacity • Required for normal emotional tone • Increase speed and amplitude of peripheral nerve reflexes
Effects Of The Thyroid Hormones On The Reproductive System • Required for normal follicular development and ovulation in the female • Required for the normal maintenance of pregnancy • Required for normal spermatogenesis in the male
Disease of thyroid gland Hypothyroidism Hyperthyroidism Graves disease (autoimmune disease) Toxic multinodular goiter Drugs (amiodarone) Thyroid storm(life threatening condition of hyperthyroidism) • Hashimoto thyroiditis (autoimmune disorder) • Iodine deficiency • Drugs (amiodarone) • Radiation exposure • Pituitary tumors • Myxedema (life threatening condition of hypothyroidism)
Hypothyroidism signs and symptoms • Symptoms and Signs or Hypothyroidism
Classification • Primary hypothyroidism is the result of • a. Gland destruction or dysfunction caused by disease or medical therapies (e.g., radiation, surgical procedures) • b. Failure of the gland to develop or congenital incompetence (i.e., cretinism) 2. Secondary hypothyroidism is the result of a pituitary disorder that inhibits TSH secretion. The thyroid gland is normal but lacks appropriate stimulation by TSH.
Classification 3. Tertiary hypothyroidism refers to a condition in which the pituitary-thyroid axis is intact, but the hypothalamus lacks the ability to secrete TRH to stimulate the pituitary. 4. Subclinical hypothyroidism refers to patients without clinical symptoms, a normal FT4, and elevated TSH levels. Currently there is insufficient evidence to support treatment because consequences of nontreatment are minimal.
Causes 1. Hashimoto thyroiditis, which is a chronic lymphocytic thyroiditis that is considered to be an autoimmune disorder 2. Treatment of hyperthyroidism, such as radioactive iodine therapy, subtotal thyroidectomy, or administration of antithyroid agents 3. Surgical excision
Causes 4. Goiter (enlargement of the thyroid gland) a. Endemic goiter results from inadequate intake of dietary iodine. This is common in regions with iodine-depleted soil and in areas of endemic malnutrition. b. Sporadic goiter can follow ingestion of certain drugs or foods containing progoitrin (L-5-vinyl-2-thiooxazolidone), which is inactive and converted by hydrolysis to goitrin. (1) Goitrins inhibit oxidation of iodine to iodide and prevent iodide from binding to thyroglobulin, thereby decreasing thyroid hormone production. (2) Progoitrin has been isolated in cabbage, kale, peanuts, brussels sprouts, mustard, rutabaga, kohlrabi, spinach, cauliflower, and horseradish. (3) Goitrogenic drugs include propylthiouracil (PTU), iodides, phenylbutazone, cobalt, and lithium. c. Less common causes include acute (usually traumatic) and subacute thyroiditis, nodules, nodular goiter, and thyroid cancer.
Treatment • Levothyroxine(L-thyroxine) • Drug of choice • Doses : • Infant and children need more • 10-15mcg\kg\day • Adults need 1.7mcg\kg\day • Old people need less than 1.7 mcg\kg\day • Pregnant need more than usual dose by 30%-50% • Must be taken before meal why? Food containing AL,Ca interfere with its absorption • TSH and T4 levels must be managed and monitored during treatment • Liothyronine • Reserved for myxedema • More cardiotoxic than levothyroxine
Levothyroxine • Clinical use : • Hypothyroidism • Prevention of mental retardation in infants with thyroid difficiency which may be avoided if it given for the first 2 wks of life • TSH suppression therapy after treatment of thyroid cancer
Levothyroxine is better than liothyronine • Longer T1\2 • 7days • Need once daily dose • Easy lab measures • Low cost • V. little risk of cardiotoxicity • Liothyronine has high risk
Side effects • Tachycardia • Heat intolerance • Tremors
Myxedema • Myxedema is a rare life threatening decompensation of hypothyroidism • Usually in individuals with long-standing hypothyroidism • Most often seen in the winter months • More common in elderly women with underdiagnosed or undertreated hypothyroidism
Myxedema • Precipitating events include • Infection • CHF • Trauma • CVA • Exposure to cold • Drugs • Sedatives • Lithium • Amiodarone
Myxedema • Treatment • No prospective studies on optimal therapy have been done thus treatment recommendations are not uniform • Airway stabilization with adequate oxygenation and ventilation or vital • Cardiovascular status must be monitored closely • Hypothermic patients should be gradually rewarmed with gentle passive external rewarming • Hypotension from reversal of hypothermic vasoconstriction should be avoided
Myxedema • Treatment cont. • Hyponatremia typically responds to fluid restrictions. Severe cases may require hypertonic saline with lasixs • Vasopressors are usually ineffective and should only be used in severe hypotension • Levothyroxine 300-500 mcg slow IVP followed by 50-100 mcg daily
Myxedema • Treatment cont. • L-triiodothyronine 25 mcg IV or orally q 8 h is a alternative • This dose should be halved in patients with cardiovascular disease • Hydrocortisone 100 mg IV q 8 hours should be given • Send baseline cortisol level to lab if possible • Precipitating causes should be sought and treated
Treatment • Thioamides • Methimazole • Propylthiouracil • Carbimazole • Iodide • Lugol’s solution • Potassium iodide • Radioactive iodine I131 • Ionic inhibitors • Perchlorate • Thiocynate • B blocker without intrinsic sympathatic activity like propranololmetoprolol • Surgery PO
Thioamides • Mechanism of action : • Inhibit peroxidase dependent reactions • Stop iodide oxidation • Stop organification • Stop coupling of thyroglobulin • Inhibit conversion of T4 to T3 in peripheral • PTU is more potent than methimazole • Major drugs used to treat hyperthyroidism • Carbimazole is converted to methimazole in vitro • Onset of action is low.why?
Comparison Propylthiouracil Methimazole Completely absorped Excretion is slower Plasma half life=6hr Once daily dosing Pregnancy category D Safe during lactation • BA=50\80% • Excretion is higher • Plasma half life =1.5 hr • 3 times dosing • Pregnancy category D • Preferred over methimazole why? • Safe during lactation