Download
1 / 1
10 likes | 154 Views
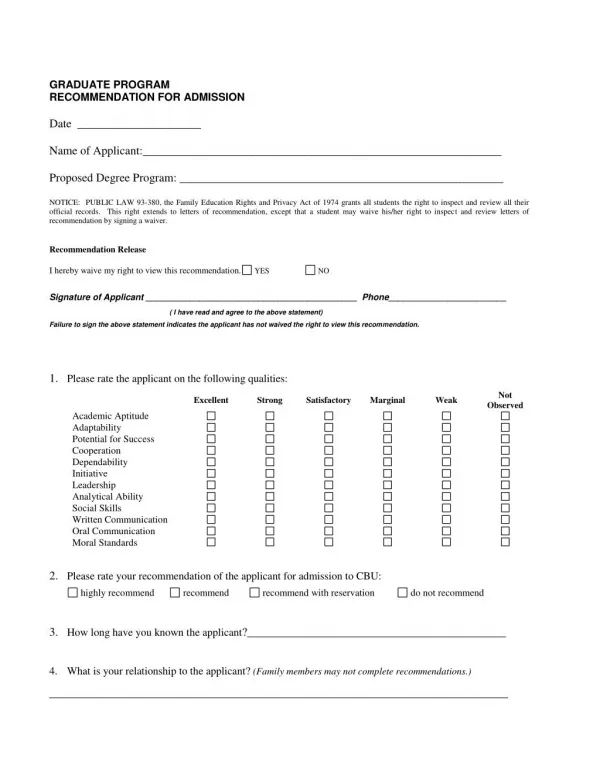
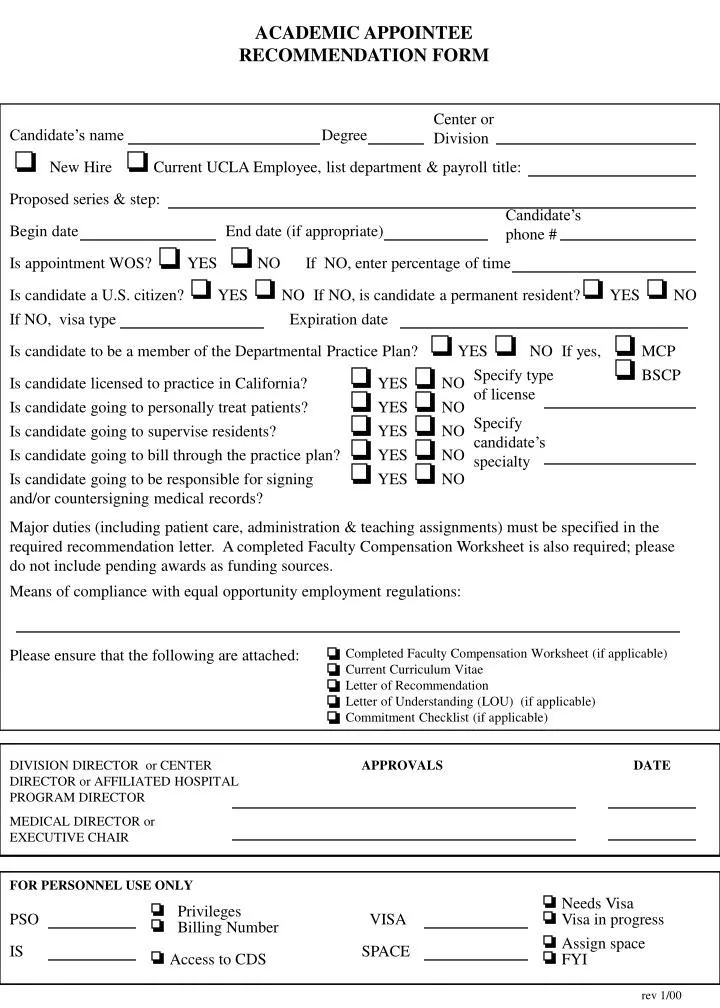
ACADEMIC APPOINTEE RECOMMENDATION FORM. Center or Division. Candidate’s name. Degree. New Hire. Current UCLA Employee, list department & payroll title:. Proposed series & step:. Candidate’s phone #. Begin date. End date (if appropriate). Is appointment WOS? YES NO.

E N D
ACADEMIC APPOINTEE RECOMMENDATION FORM Centeror Division Candidate’s name Degree New Hire Current UCLA Employee, list department & payroll title: Proposed series & step: Candidate’s phone # Begin date End date (if appropriate) Is appointment WOS? YES NO If NO, enter percentage of time Is candidate a U.S. citizen? YES NO If NO, is candidate a permanent resident? YES NO If NO, visa type Expiration date Is candidate to be a member of the Departmental Practice Plan? YES NO If yes, MCP Specify type of license BSCP Is candidate licensed to practice in California? YES NO Is candidate going to personally treat patients? YES NO Specify candidate’s specialty Is candidate going to supervise residents? YES NO Is candidate going to bill through the practice plan? YES NO Is candidate going to be responsible for signing and/or countersigning medical records? YES NO Major duties (including patient care, administration & teaching assignments) must be specified in the required recommendation letter. A completed Faculty Compensation Worksheet is also required; please do not include pending awards as funding sources. Means of compliance with equal opportunity employment regulations: Please ensure that the following are attached: Completed Faculty Compensation Worksheet (if applicable) Current Curriculum Vitae Letter of Recommendation Letter of Understanding (LOU) (if applicable) Commitment Checklist (if applicable) DIVISION DIRECTOR or CENTER DIRECTOR or AFFILIATED HOSPITAL PROGRAM DIRECTOR APPROVALS DATE MEDICAL DIRECTOR or EXECUTIVE CHAIR FOR PERSONNEL USE ONLY Needs Visa Privileges PSO VISA Visa in progress Billing Number Assign space IS SPACE Access to CDS FYI rev 1/00