Download
1 / 79
790 likes | 940 Views
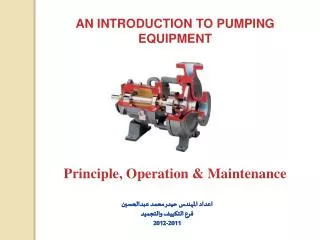
Introduction To Pumping Starting And Success. Children With Diabetes Toronto, August 17, 2007. John Walsh, P.A., C.D.E. North County Endocrine 700 West El Norte Pkwy Escondido, CA 92126 (760) 743-1431 or The Diabetes Mall (619) 497-0900 jwalsh@diabetesnet.com. Highlights. Why Pump?

E N D
Introduction To PumpingStarting And Success Children With Diabetes Toronto, August 17, 2007 John Walsh, P.A., C.D.E.North County Endocrine 700 West El Norte Pkwy Escondido, CA 92126(760) 743-1431 or The Diabetes Mall (619) 497-0900 jwalsh@diabetesnet.com Healthcare Across Borders - September 2003
Highlights • Why Pump? • Who’s A Candidate? • Pump Basics • Brands And Features • Smart Pump Advantages • Infusion Sets • How To Start • Settings That Affect Control • Wrap Up Healthcare Across Borders - September 2003
Origins • The first insulin pumps appeared in 1978 when large portable chemotherapy pumps were converted to deliver insulin • Autosyringe AS2C and Harvard Apparatus Mill Hill Infuser were early models • Used large 50 ml syringe that required users to dilute insulin to U-36 or U-18 • Had only one basal rate and no memory 1976 Biostator (top) and 1978 Autosyringe AS2C –> Healthcare Across Borders - September 2003
Reasons To Use A Pump Healthcare Across Borders - September 2003
Better Control –> Fewer Complications 76% Risk Reduction 59% Risk Reduction 39% Risk Reduction 54% Risk Reduction 64% Risk Reduction 60 • 55.0 50 Conventional Intensive Cumulative Incidence (%) 40 30 29.8 • 23.9 20 16.4 10 • 13.4 13.0 7.9 • 5.1 5.0 2.5 0 Retinopathy Laser Rx1 Micro- Albuminuria2 Clinical Progression1 albuminuria2 Neuropathy3 DCCT Research Group, Ophthalmology. 1995;102:647-661 DCCT Research Group, Kidney Int. 1995;47:1703-1720 DCCT Research Group. AnnIntern Med. 1995;122:561-568. Healthcare Across Borders - September 2003
Poor Control Remains A Problem HbA1c 2/3with diabetes (and most pumpers) remain out of control 10% Avg. A1c in TYPE 1s 9% Avg. A1c on Pumps 8% ADA 7% Goal A1c EASD/AACE 6% 5% ADA = American Diabetes Assoc., IDF = Inter. Diabetes Federation, EASD is European Assoc. for the Study of Diabetes, AACE = American Association of Clinical Endocrinologists Novo Nordisk Type 2 diabetes market research, Roper Starch Wright A., Burden et al, Diabetes Care 2002; 25:330–336 Turner RC, Cull et al, JAMA 1999; 281:2005–2012 Healthcare Across Borders - September 2003
Exposure Versus Variability One day’s tests every 30-60 min with usual meals and insulin. The DCCT proved that exposure to high blood glucose was damaging. New emphasis is on glucose variability. Variability or Swing = Standard deviation or GlycoMark test Exposure or Average = A1c or avg. BG from meter Healthcare Across Borders - September 2003
Uncontrolled A1C ~9% Time of Day The Challenge Of DiabetesBringing the A1c down smoothly takes effort 300 (16.7) “Controlled” A1C <7% BG in mg/dL (mmol) 200 (11.1) A1C ~6% 100 (5.5) Normal A1C 4%–6% 0800 1200 1800 0800 …for this you need ADVANCED therapy Healthcare Across Borders - September 2003
Advantages Of Pumps Over MDI • More reliable insulin action • Fewer missed/skipped doses • Precision – 0.05 u versus 0.5 u • Automatic dose calculations • Less insulin stacking Healthcare Across Borders - September 2003
A More Normal Lifestyle • Flexible mealtimes • Less hypoglycemia • Flexible insulin delivery for exercise, skipping meals, erratic schedules, shiftwork • Less hassle with travel and time zones • Increased sense of well being • Less anxiety while staying on schedule • Plus reminders, history, accurate dose calculations, etc.
Poor control, high A1c, wide BG excursions Nocturnal or frequent lows, hypo unawareness Frequent hospitalization/DKA Insulin sensitivity Varied or intense exercise/activity Dawn phenomenon, gastroparesis, pregnancy Varied work or school schedule, travel Insulin resistance, Type 2 diabetes Why Physicians Recommend Pumps Healthcare Across Borders - September 2003
Who Is A Pump Candidate? Healthcare Across Borders - September 2003
Candidate Requirements • Realistic expectations • Willing to monitor at least 4 times a day and keep records • Counts carbs or otherwise able to quantify food intake for meals • Willing to solve problems using diabetes management skills • Comes to clinic for follow up Healthcare Across Borders - September 2003
Expectations Healthcare Across Borders - September 2003
Benefits For Infants & Toddlers • Little ones are ideal pump candidates if parents are • Delay or split boluses for fussy eaters • Faster insulin adjustment for erratic activity • Precise dosing – 0.025 basal and 0.05 bolus – assists infants who cannot convey hypoglycemia Sxs and have frequent illnesses • Secure between shoulder blades and use lock out to avoid self dosing Back Buddy Healthcare Across Borders - September 2003
Benefits For Kids & Teens • Better for growth spurts, hormone changes in puberty, Dawn Phenomenon • Easy to cover snacks • TDD and bolus history available to ensure consistent dosing • Fast adjustments of basals and boluses for changes in activity/exercise • Lessens impact of BG swings on top of peer pressure, struggle for independence, mood swings, college, and issues with alcohol, sex, drugs Healthcare Across Borders - September 2003
Pump Basics Healthcare Across Borders - September 2003
Terms • Basal –background insulin released slowly through the day • Bolus – a quick release of insulin • Carb bolus – covers carbs • Correction bolus – lowers high readings • Bolus On Board (BOB) – bolus insulin still active from recent boluses • TDD – total daily dose of insulin (all basals and boluses) Healthcare Across Borders - September 2003
Basals And Boluses • A pump more easily matches the realities of daily life. bolus basal Healthcare Across Borders - September 2003
Basal: MDI versus Pump • Lantus or Levemir Pump 2:00 7:00 12:00 16:00 20:00 24:00 7:00 Time Basal insulin delivery from a pump provides a better and faster match for life’s needs Healthcare Across Borders - September 2003
More Testing –> Lower A1cData From 378 People On Pumps Atlanta Diabetes Associates study: 378 patients sorted from a database of 591 Pumps=MM 511 or earlier BG Target=100 C peptide <0.1 HbA1c=5.99+5.32 / (BGpd+1.39) ADA: < 7%% AACE: < 6.5% P. Davidson et al: Diabetes 53 (suppl 2): abstract 430-P, 2004 Healthcare Across Borders - September 2003
Brands And Features Healthcare Across Borders - September 2003
Insulin Pumps – 2007 • Accu-Chek Spirit • Animas 2020 • Deltec CozMore 1800 • Insulet Omnipod • Medtronic Paradigm x22 • Sooil Dana Diabecare IISG Pump info at www.diabetesnet.com/diabetes_technology/ Healthcare Across Borders - September 2003
Things To Consider In Choosing A Pump • Look, feel, color • Features: reminders, child block, waterproofing • Basal and bolus increments • Infusion set choices • Customer support • Access to history and ease of data downloads and analyses • Accessories: meter, covers, cases, PDA, smart phone Healthcare Across Borders - September 2003
Accu-Chek Spirit • Boluses based on BG not on BOB • 300 units • 0.1 u basal & bolus increments • Reversible display • Side-mounted tactile buttons • Accu-Chek Pump Configuration Software • IR (direct line) control from optional Palm PDA or smartphone • Database of 1,000 Calorie King foods in PDA Healthcare Across Borders - September 2003
Animas 2020 • High contrast color screen for easy viewing • Smallest mainstream pump • Smallest basal rate increment – 0.025 u • Waterproof – 12 ft for 24 hrs • ezCarb meal bolus calculator • ezBG correction bolus calculator • ezBolus shortcut to give bolus Healthcare Across Borders - September 2003
Deltec Cozmo • Most features: • HypoManager, Weekly Schedule, Missed Meal Bolus, Disconnect Bolus, Basal Test, Meal Maker with CozFoods, Therapy Effectiveness • Most flexible setup • Direct BG entry from attachable Freestyle meter • 300 units • 0.05 unit basal and bolus increments • Accurate bolus calculations • IR download • Best for blind or visually impaired Healthcare Across Borders - September 2003
Insulet Omnipod • No tubing for easy wear • Automatic cannula insertion and priming • 200 units • Limited to 72-80 hrs use • Watertight • Controlled by PDM or smartphone • 1000 food database Healthcare Across Borders - September 2003
Medtronic Paradigm • CGM displays BG, 3 hr trend, trend arrow, and advance warning of lows and highs • Considered least accurate CGM for detection of lows • Simple interface, less scrolling • BD meter transmits BG directly • Proprietary infusion sets • History of carbs, TDD, %basal, %carb, %correction • CareLink online software Healthcare Across Borders - September 2003
Pump + Meter Or Continuous Monitor With direct BG entry • Deltec Cozmo + Freestyle CoZmonitor • Omnipod + Freestyle • Paradigm + BD Logic • Dana Diabecare IISG With continuous monitor display • Medtronic 5/722 + Paradigm RT Planned continuous monitor displays • Abbott Navigator with Deltec Cozmo and Insulet Omnipod • Animas and Lifescan • AccuChek pump and monitor Current Feature Healthcare Across Borders - September 2003
CGM Benefits • Increased sense of security • Immediate feedback – look and learn • Improves control when used • Worth out of pocket cost for many • One unit available for about “a Starbucks a day” • Reimbursement gradually catching on Healthcare Across Borders - September 2003
Look And Learn • Excess night basal or bedtime bolus • Breakfast bolus too small or too late • Lunch bolus too small or afternoon basal too low Healthcare Across Borders - September 2003
Pump Advantages Healthcare Across Borders - September 2003
Advantages Of A Smart Pump • Automatic carb and correction calculations based on: • Preprogrammed carb and correction factors • Glucose targets • Duration of insulin action to avoid insulin stacking • Easy to check history, basal/bolus balance, and correction bolus % • Direct glucose entry from meter or continuous monitor • Helpful reminders and alerts, weekly schedule, alternate basal profiles Healthcare Across Borders - September 2003
Helps Prevent Lows • Better bolus accuracy with carb and correction factors • Less insulin stacking due to tracking BOB after boluses are given • A glucose test can reveal the current deficit – carb or insulin • Faster reduction in insulin level for exercise • Smaller pool of insulin under skin lessens risk of a large release in hot tub or weather • More predictable insulin action • Proper dosing is required! Healthcare Across Borders - September 2003
Helpful Reminders • Reminders (alarms) to • test BG after a bolus • test BG after a low reading • test BG after a high reading • give a bolus at certain time or certain period of the day • warn when bolus delivery was not completed, etc. • change infusion site • warn of low reservoir (20, 10, 5 and 0 units with an extra 10 “hidden” units for use in basal delivery) Healthcare Across Borders - September 2003
Infusion Sets Healthcare Across Borders - September 2003
Infusion Sets • Five varieties: • Self-contained (Omnipod) • Slanted Teflon • Straight-in Teflon • Slanted metal • Straight-in metal • Three connections: • Luer lock pumps: ~ 25 varieties • Paradigm: ~ 4 varieties • Omnipod: 1, auto-inserted A reliable and comfortable infusion set is critical to success on a pump. Healthcare Across Borders - September 2003
Infusion Sets And InsertersInfusion set/site problems are a common cause for unexplained highs Disetronic Rapid-D Smith’s Medical Cleo Medtronic Sil-serter Quik-serter Animas Inset Healthcare Across Borders - September 2003
Use Sterile Technique For Site Prep • 30% of people are constant staph carriers and 25% are intermittent. MRSA is now common. Prevent infections: • Wash hands • Sterilize skin with IV Prep • Place bio-occlusive IV3000 over site • Insert infusion set through IV 3000 Steps for staph carriers: • Use antiseptic soap all over body once every 1-2 weeks • Occasionally, apply bacitracin ointment to inside of nose Healthcare Across Borders - September 2003
Tape The Tubing!!! • One inch tape over the infusion line stops tugging • Tape stops tunnelling – movement of teflon nder skin allows insulin to tunnel to the surface, causing unexplained highs • Less skin irritation from movement • Prevents pull outs At tug time, lose tape not insulin! Photo courtesy of kerri@sixuntilme.com Healthcare Across Borders - September 2003
Pump Start Healthcare Across Borders - September 2003
Prepare For Pump Start • Use basal/bolus approach first with injections • Use accurate carb counts • Read Pumping Insulin and pump manual • Practice with your pump as soon as it arrives • View CD/DVD as you practice with your pump • Get training in pump operation andtroubleshooting Healthcare Across Borders - September 2003
Preparation Ask how to discontinue your long-acting insulin Determine start-up settings for TDD, basal/bolus balance, carb and correction factors, and DIA • Get prescriptions for insulin, test strips, IV Prep, IV 3000 dressings, etc. • Have contacts for MD, CDE, pump company, pump rep, other pumpers Healthcare Across Borders - September 2003
Steps To Success • Test often • Keep great records (Smart Charts, download, etc) • Take a bolus for every bite • except when carbs are used to raise a low BG • or when eating to compensate for exercise • Take boluses early • Write down a reason for every high and low • Change infusion site on schedule and whenever unexpected highs occur Healthcare Across Borders - September 2003
Steps To Control • Stop lows first • Set a realistic DIA • Determine an optimum TDD • Set and test basals • Determine starting carb factor with 450 Rule (450/TDD) and correction factor with 2000 Rule (2000/TDD) • Periodically check basal/bolus balance • Look for and correct unwanted patterns Healthcare Across Borders - September 2003
Stop Lows FirstBetter control and more stability • Mild lows cause followup lows • Small epinephrine release makes muscles sensitive to insulin • Can lead to another low as much as 36 hours after the first • More carbs than usual are needed Severe lows cause highs Higher stress hormone release makes glucose rise for 6-10 hrs Excess carb intake leads to highs Boluses may be reduced/skipped More insulin than usual needed To stop lows, lower the TDD!!! Healthcare Across Borders - September 2003
Find Your Optimum Doses! • Start with an accurate TDD – • 1. How much total insulin do you average a day? • 2. Adjust the TDD – are highs or lows primary problem? • Stay in basal/bolus balance – 50/50 or 45-65% as basal • Use the 500 and 2000 Rules to estimate starting carb and correction factors • Then adjust your basal and bolus doses • TEST your blood glucose • LOOK for blood sugar patterns • ADJUST basals and boluses from your patterns Healthcare Across Borders - September 2003
Find Basals And Boluses From Starting TDD Starting Carb Factor Corr. Factor TDD 50% Basal 500 Rule 200 Rule 20 u 0.42 u/h 25 grams 100 mg/dl 25 u 0.52 u/h 20 grams 80 mg/dl 30 u 0.63 u/h 17 grams 67 mg/dl 35 u 0.73 u/h 14 grams 57 mg/dl 40 u 0.83 u/h 13 grams 50 mg/dl 50 u 1.04 u/h 10 grams 40 mg/dl 60 u 1.25 u/h 8 grams 33 mg/dl 3.1 mmol An accurate TDD solves most control problems! Healthcare Across Borders - September 2003
Duration Of Insulin Action (DIA) Time An accurate DIA time is critical to success on a smart pump Current research suggests that DIA times are NOT different between children and adults • Shorter for those more sensitive to insulin, but NOT children in general But immediate factors can affect insulin action time: • Shorter with activity and exercise • Shorter in hot weather • Longer with fat in diet Healthcare Across Borders - September 2003