Download
1 / 54
550 likes | 1.64k Views
Discover the history and evolution of kidney transplants, immunosuppression techniques, drug categories, and potential side effects. Learn about induction agents, maintenance therapies, and monitoring processes to ensure successful transplantation outcomes.

E N D
History 1909 - The first kidney transplant experiments were performed in humans in France using animal kidneys (rabbit). 1933 - The first human-to-human kidney transplant was performed. 1954 - The first successful human-to-human transplant from one twin to another by Dr. Joseph E. Murray and his colleagues at Peter Bent Brigham Hospital in Boston. 1962 – The first cadaveric donor kidney transplant at Peter Bent Brigham Hospital (now Brigham & Women's Hospital) in Boston.
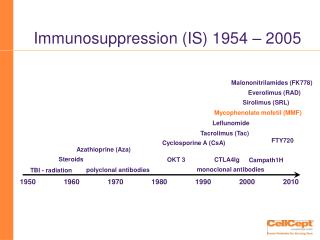
General Principle of Immunosuppression Primary immune responses are more easily repressed than secondary (memory) Suppression is more likely to be achieved if therapy is begun before exposure to the immunogen Different immunosuppressants have different effects on different immune reactions and mediators
Introduction Advances in transplant immunosuppression have contributed to the decrease in the frequency of acute rejection increase in graft survival longevity for renal allograft recipients Proliferation of agents means more options different mechanisms of action more complicated management schemes increase potential for drug-drug interactions and complex side effect profiles
Categories of Agents Induction agents Monoclonal or polyclonal antibodies Administered intravenously immediately following surgery Maintenance agents Prednisone CNIs form the cornerstone of immunosuppressive therapy Antiproliferative agents: Cellcept, Imuran, Rapamune Triple agents / withdrawal / avoidance / conversion
Immunologic History Sensitization First or re-transplant Rejection Infection HLA-matching
Induction Agents Muromonab (OKT3) Equine polyclonal ATG (ATGAM) Rabbit polyclonal ATG (Thymoglobulin) Basiliximab (Simulect) Daclizumab (Zenapax) Alemtuzumab (Campath-1H) FTY 720
Induction Thymoglobulin 1ST dose given in OR Dose: 1.5 mg/kg Total dose: usually 6 mg/kg Adverse effects: cytokine release syndrome (fever, chills, arthralgia), leucopenia, thrombocytopenia Premedication: Tylenaol, Benadryl, Hydrocortisone Also effective in treating rejection
Induction Anti-IL-2 Receptor Antibodies Basiliximab (Simulect) Daclizumab (Zenapax)
Anti-IL-2 Receptor Antibodies Basiliximab (Simulect) Chimeric antibody (75% human, 25% mouse) Dosing: 20 mg i.v. pre-op and POD# 4 Daclizumab (Zenapax) Humanized (95% human, 5% mouse) Dosing: 1 mg/kg pre-op and q 2 w for total 6 doses Not effective for treating rejection
Calcineurin Inhibitors Cyclosporine Different preparation are not equivalent Sandimmune (cyclosporine, USP) Gengraf (cyclosporine, USP – Modified) Neoral (cyclosporine, USP – Microemulsion) Tacrolimus (FK 506, Prograf)
Advantages of CsA Microemulsion formulation Twice the bioavailability Less intraindividual and interindividual variability Reduced time (more than 30 percent) to maximal concentration (Tmax) Absorption and drug levels are less susceptible to the effects of food (particularly fatty foods), Not dependent upon bile salts for absorption.
CNI: Dosing Cyclosprine (Neoral, Gengraf, Sandimmune) Initial dosing: 8-10 mg/kg/day Maintenance: 2-6 mg/kg/day Tacrolimus (Prograf) Initial dosing: 0.15 mg/kg/day Maintenance:0.05-0.15 mg/kg/day
Cyclosporin: Monitoring Trough or C0 level S Hariharan. Am J Kidney Dis. 2006. 47(S2):S22-S36.
Cyclosporin: Monitoring Cyclosporin: C2 Level < 6 months: 1000-1500 ng/ml > 6 months: 800-900 ng/ml Little evidence from prospective studies to support the theoretical benefits of C2 monitoring. Potential dose reductions in stable patients may reduce costs, but no short-term clinical benefit is seen.* *Knight, S R. et al. Transplantation 2007 Jun; 83(12):1525-1535
Tacrolimus (Prograf): Monitoring S Hariharan. Am J Kidney Dis. 2006. 47(S2):S22-S36.
CNI Side Effects Nephrotoxicity (Striped fibrosis) TMA Type IV RTA
Metabolic Interactions That Increase CNI Levels Calcium channel blockers Verapamil Diltiazem Amlodipine Nicardipine Antifungal agents Ketoconazole Fluconazole Itraconazole Clotrimazole Metronidazole Immunosuppressants Sirolimus Glucocorticoids Methylprednisolone Antibiotics Erythromycin Clarithromycin Josamycin Ponsinomycin Azithromycin Protease Inhibitors Saquinavir Indinavir Nelfinavir Ritonavir Foods Grapefruit Grapefruit juice
Metabolic Interactions That Decrease CNI Levels Antituberculosis drugs Rifampin Rifabutin Isoniazid Anticonvulsants Barbiturates Phenytoin Carbamazepine Herbal preparations Saint John’s wort Antibiotics Nafcillin IV trimethoprim IV sulfadimidine Imipenem Cephalosporines Terbinafine Ciprofloxacin Other drugs Ticlopidine Octreotide Nefazodone
CNI Tacrolimus v. Sandimmune acute rejection may be less with tacrolimus. similar graft survival Tacrolimus v. Neoral In some studies, tacrolimus has reportedly had lower acute rejection rates. Despite this, both agents are associated with similarly excellent allograft survival rates, although some studies report an advantage of one agent over the other.
CNI In a meta-analysis and meta-regression study of 123 reports from 30 trials (4102 patients), the followings were found. At six months, graft loss was significantly reduced in tacrolimus treated recipients and this effect persisted up to three years. At one year, tacrolimus treated patients had less acute rejection. Treating 100 recipients with tacrolimus instead of cyclosporin for the first year after transplantation avoids 12 patients having acute rejection and two losing their graft but causes an extra five patients to develop insulin dependent diabetes. Webster AC. Et al. BMJ 2005 Oct 8;331(7520):810
Dosing of Adjuvant Agents *Borrows R, et al. Am J Transplant 2006(6):12-128
Antiproliferative Agents *Borrows R, et al. Am J Transplant 2006(6):12-128
Myfortic Enteric-coated MMF Intended to reduce GI side effects but has not been proved in clinical trials Dose equivalent 180 mg Myfortic = 500 mg MMF
Mycophenolate v. Azathioprine Several studies, particularly some initial pivotal reports, found that acute rejection rates were lower with mycophenolate. However, these studies may be flawed. Given current evidence, azathioprine and mycophenolate mofetil appear to be similar in terms of acute rejection rates and long-term allograft survival rates.
Mycophenolate v. Azathioprine MYSS Trial 336 patients undergoing a deceased donor renal transplant randomly assigned to mycophenolate mofetil or azathioprine both groups also receiving cyclosporine microemulsion and corticosteroids. Corticosteroids were continued for the first six months (phase A), after which they were slowly withdrawn and patients were followed for another 15 or more months (phase B). Remuzzi G. et al. Lancet 2004 Aug 7;364(9433):503-12.
Mycophenolate v. Azathioprine MYSS Trial The incidence of clinical rejection was the same for both mycophenolate and azathioprine in phase A (34 and 35 percent, respectively) and phase B (16 and 12 percent, respectively). Rates of allograft loss, and serum creatinine concentration were the same in both groups. However, mycophenolate was approximately 15 times more expensive than azathioprine Remuzzi G. et al. Lancet 2004 Aug 7;364(9433):503-12.
Mycophenolate v. Azathioprine MYSS Follow-up Study Remuzzi G. et al. J Am Soc Nephrol. 2007 June; 18: 1973–1985.
Mycophenolate v. Azathioprine the long-term risk/benefit profile of MMF and azathioprine therapy in combination with cyclosporine Neoral is similar. In view of the cost, standard immunosuppression regimens for kidney transplantation should perhaps include azathioprine rather than MMF.
mTOR Inhibitor Sirolimus (Rapamune / Rapamycin) Dosage: 2-5 mg qd Level: 5-15 ng/mL (whole blood trough level)
Drug Interactions With Sirolimus As sirolimus is metabolized by the same pathway as the CNIs (P-450 3A4), interactions are the same Sirolimus has been shown to raise blood levels of cyclosporine and MMF Sirolimus should be administered 4 hours after cyclosporine or tacrolimus Sirolimus blood levels are raised by cyclosporine Proper monitoring is advised
Steroids • Prednisone • Methylprednisone • Decreased activity with anti-TB and anti-seizure medications • Increased activity with estrogen, OCP, erythromycin