Download
1 / 28
280 likes | 432 Views
Eight M onths A ngiographic F ollow-up in P atients R andomized to Crush or Culotte S tenting of C oronary A rtery B ifurcation L esions The Nordic Bifurcation Stent Technique Study.

E N D
Eight Months Angiographic Follow-upin Patients Randomized to Crush or CulotteStenting of Coronary Artery Bifurcation LesionsThe Nordic Bifurcation Stent Technique Study PålGunnes, MattiNiemela, Kari Kervinen, AndrejsErglis, IndulisKumsars, Jens F Lassen, Michael Mæng, Jan Skov Jensen, Anders Galløe, TerjeSteigen, Jan Ravkilde, TimoMakikallio, Kari Ylitalo, Inga Narbute, Evald Christiansen, Lars Krusell, SindreStavnes, UlrikAbildgaard, Peter Riis Hansen, Jan Mannsverk, Thor Trovik, Per Thayssen, Steffen Helqvist, SailaVikman, Rune Wiseth, Jens Aarøe, Leif Thuesen For the Nordic-Baltic PCI Study Group
None of the authors had disclosures with regard to the present study
Nordic-Baltic PCI Study Group: independent working group of interventional cardiologists in the Nordic and Baltic countries The Cypher Select stents used in this study were purchased at market price An unrestricted grant of €625 was donated by Cordis JJ to the participating hospitals per randomized patient The Nordic Bifurcation Stent Technique Study
Denmark Aarhus University Hospital, Skejby (83 pts) Gentofte University Hospital (44 pts) Odense University Hospital (14 pts) Rigshospitalet, Copenhagen (11 pts) Aalborg University Hospital (3 pts) Latvia Paul Stradins Hospital, Riga (92 pts) Finland Oulu University Hospital (87 pts) Helsinki University Hospital (11 pts) Tampere University Hospital (8 pts) Kuopio University Hospital (2 pts) Norway Feiring Heart Clinic (50 pts) Tromsø University Hospital (15 pts) St Olav Hospital, Trondheim (4 pts) Participating Centres
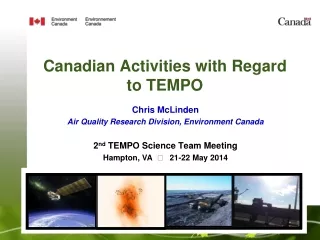
Purpose In a randomized trial to compare • CRUSH • CULOTTE bifurcation stenting techniques using sirolimus-eluting stents
Crush-stenting Culotte-stenting
Inclusioncriteria • Stable or unstable AP or silent ischemia • Bifurcation lesion of LAD/diagonal, Cx/obtuse marginal, RCA-PDA/posterolateral branch or LM/Cx/LAD in a right dominant system • Diameter of main vessel by visual estimate >3.0 mm • Diameter of side branch by visual estimate >2.5 mm
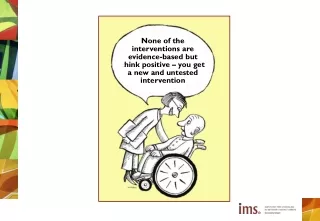
Randomization (n: 424) CULOTTE (n: 215) CRUSH (n: 209) n: 424 (100%) Clinical Follow up, 6 months (n: 215) Clinical Follow up, 6 months (n: 209) n: 424 (100%) Stratification at randomization Scheduled Angiographic Follow up, 8 months (n:189) Scheduled Angiographic Follow up, 8 months (n: 184) n: 373 (88%) Angiographic FU available (n: 160) Angiographic FU available (n: 164) n: 324 (87%)
Randomization (n: 424) CULOTTE (n: 215) CRUSH (n: 209) n: 424 (100%) Clinical Follow up, 6 months (n: 215) Clinical Follow up, 6 months (n: 209) n: 424 (100%) Stratification at randomization Scheduled Angiographic Follow up, 8 months (n:189) Scheduled Angiographic Follow up, 8 months (n: 184) n: 373 (88%) Angiographic FU available (n: 160) Angiographic FU available (n: 164) n: 324 (87%)
Angiographic end points • In-lesion >50% stenosis of the entire bifurcation • In-stent >50% stenosis of the entire bifurcation • In lesion >50% stenosis of MV • In lesion >50% stenosis of SB • Late loss of MV and SB
Baseline demographics CRUSHCULOTTE p-value (n=160) (n=164) Age (yrs) 65 64 ns Male sex (%) 76 75 ns Diabetes (%) 14 15 ns Smoker (%) 23 31 ns Hypertension (%) 63 64 ns Statin tx (%) 84 73 0.02 Family history (%) 54 62 ns History of PCI (%) 46 35 0.05 History of CABG (%) 3 6 ns
Vessels treated CRUSH (n=160) CULOTTE (n=164) 10% 11% 5% 8% 16% 19% 62% 68% ns
Procedural data CRUSH CULOTTE p-value (n=160) (n=164) MV stented (%) 100.0 99.4 ns SB stented (%) 99.4 97.0 ns Kissing balloon (%) 88.8 93.9 ns Tx successful* (%) 98.8 100.0 ns * (Residual stenosis <30% of MV + TIMI flow III in SB)
Patients with true bifurcation lesion Medina classification 1,1,1 - 1,0,1 - 0,1,1 CRUSH CULOTTE p-value (n=160) (n=164) True bifurcation 125 (78%) 140 (85%) ns
Quantitative coronary angiography (QCA) Computer-based system dedicated to bifurcation analysis (Qangio XA version 7.0, Medis, Leiden, The Netherlands) Angiographic core labs: • Aarhus University Hospital, Skejby, Denmark • Paul Stradins Clinical Hospital, Riga, Latvia
Angiographic follow-up after 8 months Complete angiographic evaluation in 324 (87%) patients MV prox SB • QCA measurements in: • Proximal main vessel • Distal main vessel • Side branch • Edge (5 mm) MV dist
Reference diameter (mm)before procedure mm ns ns ns
Rate of mainvesseland/or side branch in-lesion diameter stenosis >50% at 8 monthsfollow-up % 12.1 p=0.10 6.6
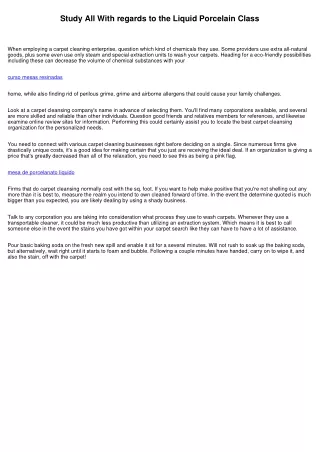
Rate of main vessel and/or side branch in-stent diameter stenosis >50% at 8 months follow-up % 10.5 p=0.046 4.5
Rate of mainvessel in-lesion diameter stenosis >50% at 8 monthsfollow-up % p=0.19 4.7 2.0
Rate of side branch in-lesion diameter stenosis >50% at 8 months follow-up % p=0.10 9.2 4.5
Localization of in-stent restenosisat 8 months follow-up CRUSH CULOTTE 0.0% 0.0% 3.8%* 9.8%* 0.6% 2.0% * p=0.04
Localization of edge restenosisat 8 months follow-up CHRUSH CULOTTE 0.0% 2.0% 2.0% 1.3% 1.3% 0.7%
In-stent late lumen loss (mm) mm ns ns ns
Conclusion • CRUSH and CULOTTE bifurcation stenting using sirolimus eluting stents were associated with low rates of restenosis at eight months angiographic follow-up • The few restenoses were primarily located in side branches treated with the CRUSH technique • The CULOTTE bifurcation stenting technique was associated with a single digit restenosis rate and may be preferred in suitable bifurcation anatomies • Extended follow-up needed to evaluate the safety of the investigated two-stent bifurcation techniques