Download
1 / 13
130 likes | 318 Views
Adherence, attitude to Standard Treatment Guidelines in clinical practice at tertiary care hospitals in Delhi State. 1 Sangeeta Sharma, 2 Sharma KK, 3 Sethi GR, 4 Sachdev GK, 5 Dwivedi S, 6 Faridi MAA

E N D
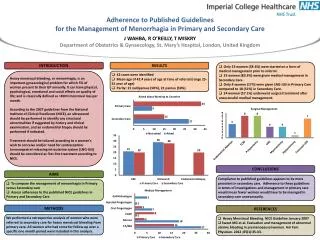
Adherence, attitude to Standard Treatment Guidelines in clinical practice at tertiary care hospitals in Delhi State 1Sangeeta Sharma, 2Sharma KK, 3Sethi GR, 4Sachdev GK, 5Dwivedi S, 6Faridi MAA 1Department of Pharmacology, Institute of Human Behaviour & Allied Sciences, Department of 2Pharmaoclogy, 5Medicine, 6Paediatrics, University College of Medical Sciences, Department of 3Paediatrics, 4Medicine, Maulana Azad Medical College, Delhi, India
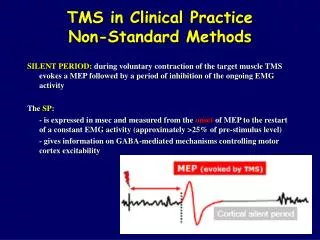
Abstract Problem Statement: Substantial efforts have been devoted to improving rational use of drugs byphysicians and compliance with best practices. Comprehensive Standard Treatment Guidelines (STGs) were developed to assist this process. Objectives: To evaluate the effectiveness of STGs on the quality of prescribing and medical care, explore physicians’ attitudes and reasons for not following treatment guidelines, and to mount an effective intervention strategy to improve adherence to guidelines. Design: Prospective, pre-post intervention design with a control group and a qualitative study using a semi- structured questionnaire. Setting and Population: Medicine and paediatric departments at two tertiary care hospitals. One hundred prescriptions each for five tracer diseases, namely acute upper respiratory infection (AURI), diarrhoea, malaria, hypertension and asthma were collected between 2002-2003 at baseline, i.e., before dissemination of STGs and at 1, 3, and 6 months after dissemination. Intervention: The interventions consisted of advocacy and dissemination of STGs to both study sites. In addition, educational intervention was undertaken after dissemination of the STGs to reinforce acceptance of STGs comprising prescription review feedback, reminders and small group discussions focussing on new approaches for understanding factors related to physicians adoption of guidelines in clinical practice. Outcome Measures: Core drug use indicators: Average number of drugs/case; % of generic drugs; % of drugs on the Essential Drugs List (EDL); % of patients receiving antibiotics; and % adherence to STGs. Results: At baseline, the extent of compliance with STGs was low: (39% vs. 30.5%) and a considerable proportion of prescriptions (27% vs 22%) were either wrong or dubious in both control and study groups. Percent adherence to STGs improved in the both groups following advocacy and distribution of STGs but was significant (P<0.01) in the intervention health facility. Rates of use of essential drugs were high, with 80-90% actually dispensed in both the groups. Most doctors welcomed the STGs but find it difficult to adopt. External factors such as lack of organizational support, practice environmental factors (heavy patient load, complexities in clinical presentation), and professional characteristics (seniority and specialist practice) were frequently offered as reasons for non-compliance. Conclusions: The existence of the guidelines alone does not ensure compliance. Continuing advocacy efforts and intensive interactions are required to improve adoption of the guidelines and also to attend to environmental factors and organizational support systems.
Aims & Objectives • Multifaceted implementation is associated with increased uptake of the Standard Treatment Guidelines (STGs). The STGs have been introduced through an official launch and distributed to all the doctors. • The aims & objectives of the present study were: • To evaluate the extent of adherence to STGs before and after introduction of STGs and effectiveness of STGs & educational education on the quality of prescribing. • To find out the acceptance and attitude towards Standard Treatment Guidelines by prescribers.
Methodology • Pre-post intervention (after one month, three months and six months) study design with a control group • Study sites: Medicine & Paediatrics department at two tertiary care teaching hospitals – • GTB and LN Hospital Methodology • Hundred prescription for each of the five tracer diseases namely • Acute upper respiratory infection (AURI), Diarrhoea, Malaria, Hypertension, Asthma. • Study duration 2002-2003
Methodology • Attitude of the prescribers towards clinical guidelines: • Seven items questionnaire on attitude to guidelines was used as a means of evaluation of the attitude and focusing discussion • Questionnaire was administered to 26 and 23 doctors at the intervention and control health facility respectively
Outcome measures • The choice of drug and adherence to the STG was scored on a 4 point scale • Score 3: Drugs prescribed as per guidelines • Score 2: Alternatives other than in EDL prescribed • Score 1: Unnecessary drugs which have no role prescribed • Score 0: Contraindicated drugs or incompatible combination prescribed • Core drug use indicators • Average number of drugs per encounter • Percentage of drugs prescribed by generic name • Percentage of drugs prescribed from essential drugs list • Percentage of drugs actually dispensed • Completeness of prescription • Score was given for dosage form, strength, frequency, duration of treatment.Score 4: all parts; Score 3: three parts; Score 2 two parts; Score 1: only one part mentioned
Intervention The interventions consisted of: • Advocacy and dissemination of STGs to both study sites. • Two educational interventions were undertaken separately for junior doctors and consultants to reinforce acceptance of STGs • Prescription review feedback & reminders • Small group discussions focussing on new approaches for understanding factors related to physicians adoption of guidelines in clinical practice.
Overall adherence to STGs n= 472 n= 376 n= 406 n= 377 Control Health facility
Overall adherence to STGs * p<0.01 n= 515 n= 480 n= 480 n= 372 Intervention Health facility
Completeness of prescription Control Intervention
Results • Junior doctors welcomed the suggestion of having STGs. • Most senior doctors (consultants) agreed that STGs improve the quality of care but find it difficult to adopt and external factors were frequently offered as reasons for non-compliance such as • Lack of organizational support • Practice environmental factors (heavy patient load, Complexities in clinical presentation) • Professional characteristics (seniority and specialist practice).
Conclusion • Prescriptions for essential drugs & percent drugs dispensed were high in both control & intervention group. • Prescribing by generic names is low • Adherence to STGs improved significantly in the intervention health facility. • The existence of the guidelines alone does not ensure compliance. • Continuing advocacy efforts and intensive interactions are required to improve adoption of the guidelines and also to attend to environmental factors and organizational support systems.