Download
1 / 47
530 likes | 957 Views
Screening for P reeclampsia and IUGR . Prof Dr Rıza Madazlı Istanbul University Cerrahpaşa Medical Faculty. Pre-eclampsia. %2-7 M ajor cause of maternal and perinatal mortality and morbidity 50 000 maternal death/year ¼ of obstetric admissions to intensive care units.

E N D
Screening for Preeclampsia and IUGR Prof Dr Rıza Madazlı Istanbul University Cerrahpaşa Medical Faculty
Pre-eclampsia • %2-7 • Major cause of maternal and perinatal mortality and morbidity • 50 000 maternal death/year • ¼ of obstetric admissions to intensive care units
Fairly restricted to humans • Pregnancy specific / PLACENTA • Brain is energetically expensive and requires adeeply invasive placenta / RISKY PROCESS • Cost of Evolution / To be human • Discover secrets of pregnancy
Maternal Syndrome / Endothelial Dysfunction • All clinical manifestations can be explained by endothelial dysfunction
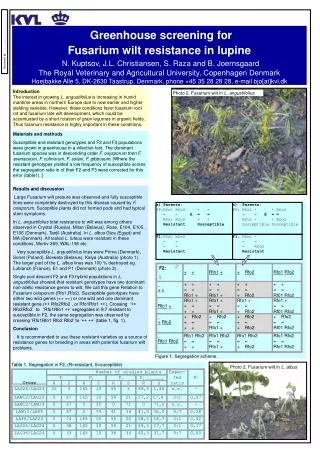
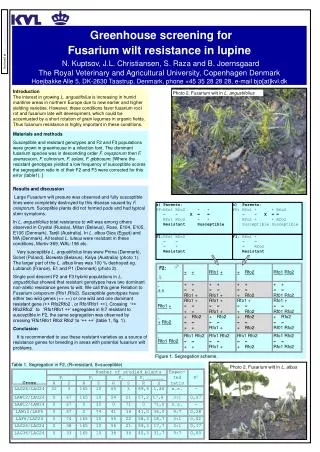
Placentation - Inadequate Trophoblastic Invasion Madazlı et al, BJOG, 2000
ImmuneGeneticTrophoblastic MaladaptationPredisposition Defect Placentation Defect Cytokines Leukocyte Activation Lipid Peroxidation Apoptosis/ Microparticule Compleman Activation Maternal Endothelial Dysfunction Pre-eclampsia
Early and Late PE • Associated with different • Maternal and fetal outcomes • Biochemical markers • Heritability • Clinical features • Predictability • Have different etiologies • Differentforms of the disease
Late Onset PE • (≥34 GW) • Early Onset PE • (<34 GW) • Placental PE • Abnormal UtA Doppler • High FGR • Highfetal andmaternal mortality, morbidity • Maternal PE • NormalUtA Doppler • Low FGR • Perinatal outcome favourable • Exaggerated systemic inflamatory response
Screening Placentation • Disease • 1. Trm • 3. Trm • Prediction • Early diagnosis • Preclinic diagnosis
Prophylactic low-dose aspirin < 16 weeks • reducesthe prevalence by about 50% • reduce the prevalence of preterm PE byabout 90% • no significant effect on the risk of term PE
Screening at 11–13 weeks • define the high-risk group for prophylactic treatment with low-dose aspirin • Screening at 20–24 weeks • improve the prediction provided by the firsttrimesterassessment • closer surveillanceof the maternal and fetal condition • define the best time for delivery
Biochemical markers • products of trophoblast or decidua and reflect the placental dysfunction • inflammatory or metabolic responses of maternal systems to abnormal pregnancy • Maternal Characteristics • BMI • MAP • Uterine Artery Doppler
Maternal Characteristics +LR • Age >40 1.96 • Nulliparous 2.91 • Previous PE 7.19 • Family history of PE 2.90 • Multiple pregnancy 2.83 • APL Syndrome 9.72 • Diabetes 3.56 • Chronic hypertension ↑ • SLE ↑ • DR 30- 45% / FPR 10–25% • Morethan ½ the women develop pre-eclampsia have norisk factors
BodyMass Index (BMI) • BMI ≥25 BMI ≥35 • Sensitivity 47% (33–61) 21% (12–31) • Specificity 73% (64–83) 92% (89–95) • +LR 1.7 (0.3–11.9) 2.7 (1.0–7.3)
Mean arterial pressure (MAP) +LR • MAP>90mm Hg 3.5 • 10% FPR, DR 37.5% MAP • Poon, Hypertension. 2008 • Cnossen, BMJ,2008
Biochemical markers • Endothelial Dysfunction • Fibronectin • PTX3 • Selectin • Oxidative stress markers • Insulin resistance • TNF-α • SHBG • Adiponectin • Leptin • Genomic, Metabolomics • C-free DNA • AngiogenicProteins • PIGF • VEGF • sFLT1 • sENG • Serum Analytes • HCG • PAPP-A • AFP • uE3 • İnhibin • ADAM12 • PP13
AngiogenicProteins (Factors) • Placental growth factor (PlGF) ↓ • Vascular endothelial growth factor (VEGF) ↓ • Solublefms-like tyrosine kinase-1 (sFLT1) ↑ • Soluble endoglin (sENG) ↑ • imbalance in circulating angiogenic factors
sFLT1 • 17 studies • PlGF • 18 studies
sENG - 9 studies • Test accuracy is too poor for accurate identificationin clinical practice • Should not be used alone for the prediction of pre-eclampsia.
PIGF Andraweera et al. VEGF family in adverse pregnancy outcomesHuman Reproduction Update, 18, 436–457, 2012
Downs Screening • HCG ↑ • PAPP-A ↓ • AFP↑ • uE3 ↓ • İnhibin ↑
Placental protein 13 (PP13) • First trimester PP13 inadequate for screening
Uterine Artery Doppler Madazlı et al, Placenta, 2003
Second Trimester UtA Doppler • PE • +LR : 7.5 • FGR • overall (+LR: 9.1) • severe (+LR: 14.6)
Useful for predicting early-onset pre-eclampsia, aswell as other adverse pregnancy outcomes • AbnormalUtA Doppler in low-riskwomen sufficiently high performance to justifyaspirin prophylaxis
Screening at 11–13 weeks / Prophylaxis • Combination tests more effective • More effective / Early onset preeclampsia