Download
1 / 21
300 likes | 1.55k Views
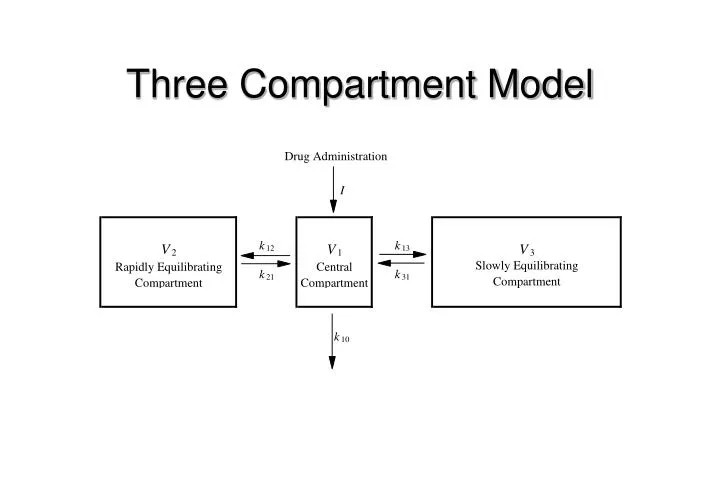
Three Compartment Model. Remifentanil vs. other opioids. 100. 10. Percent of peak plasma opioid concentration. fentanyl. 1. sufentanil. alfentanil. remifentanil. 0.1. 360. 480. 600. 240. 0. 120. Minutes since bolus injection. Minto et al, Anesthesiology, in press.

E N D
Remifentanil vs. other opioids 100 10 Percent of peak plasma opioid concentration fentanyl 1 sufentanil alfentanil remifentanil 0.1 360 480 600 240 0 120 Minutes since bolus injection Minto et al, Anesthesiology, in press
Remifentanil vs. other opioids 100 sufentanil 80 fentanyl 60 Percent of peak effect site opioid concentration 40 alfentanil 20 remifentanil 0 4 6 8 10 0 2 Minutes since bolus injection Minto et al, Anesthesiology, in press
V1 and Clearance decrease with age • V1 decreases about 20% from age 20 to 80 • Common finding for anesthetic drugs • Clearance decreases about 30% from age 20 to 80 • Mechanism unknown
EC50 decreases with age • EC50 is a measure ofbrain sensitivity • Decreased EC50 means increased sensitivity • Decreased EC50 with age also reported for: • fentanyl • alfentanil • sufentanil
t 1/2 ke0 increases with age • t 1/2 ke0 is the time required for the brainto equilibrate withthe plasma • an increase in t 1/2 ke0would be expected toresult in a slower onsetof drug effect
Bolus doses should be reduced by 50% in the elderly • The reduction in bolus dose is because of the 50% increase in sensitivity in the elderly • Adjusting the bolus for age is at least as important as adjusting it for body weight
Age effects on bolus dose Minto et al, Anesthesiology, in press
Infusion rates should be reduced by 2/3’s in the elderly • The infusion rate is decreased because of increased sensitivity and decreased clearance • Adjusting the infusion rate for age is more important than adjusting it for weight
Age effects on infusion rate Minto et al, Anesthesiology, in press
Age affects variability in time to emergence Minto et al, Anesthesiology, in press
Hemodynamics in Elderly • Blood pressure may decrease 10-40 percent in elderly (>70 yrs). • Easily treated with ephedrine. • May be associated with ST changes if patient has coronary artery disease.
Hemodynamics in Elderly • Heart rate is usually stable but may increase abruptly on emergence. • May be associated with ST changes if patient has coronary artery disease
Propofol/Alfentanil Interaction • Adapted from Vuyk et al, Anesthesiology 83:8-22, 1995 • Characterizes the concentrations for • intubation • maintenance • on emergence • Concentrations are 50% response level