Download
1 / 40
470 likes | 1.35k Views
Insulin Use In Outpatient and Inpatient Settings. Greg Cook, MD Endocrinology Fellow. Objectives. Become familiar with different types of insulin and their actions Understand how various insulin regimens compare and contrast with endogenous insulin production

E N D
Insulin Use In Outpatient and Inpatient Settings Greg Cook, MD Endocrinology Fellow
Objectives • Become familiar with different types of insulin and their actions • Understand how various insulin regimens compare and contrast with endogenous insulin production • Become comfortable initiating and managing insulin in the outpatient setting • Learn basics of inpatient insulin therapy • Learn how to use insulin to help address hyperglycemia caused by glucocorticoids or enteral nutrition
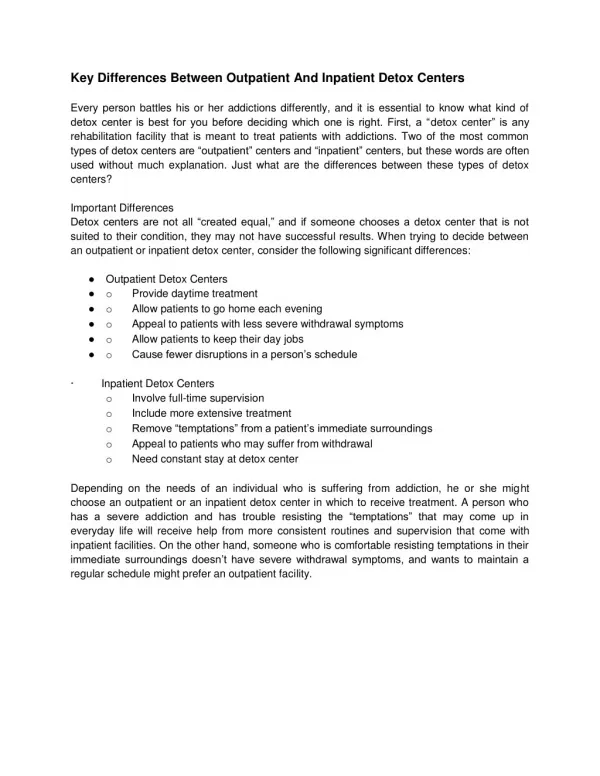
Case I 45 yo man with 12 year history of DM type II presents for initial visit to outpatient clinic. He is currently on metformin 1 gram BID and glipizide 10mg BID. He monitors his glucoses infrequently and reports fasting values of 200-250. His mother recently died from diabetic complications, and he is very concerned about developing similar problems himself. Exam: Wt 242 lb (110 kg), BP is controlled Obese, +acanthosis nigricans on neck Labs: Serum glucose 286, Cr 1.3, Hgb A1c 9.6 In addition to encouraging dietary and lifestyle changes, how would you manage his diabetes?
Acanthosis Nigricans Derm Atlas – www. dermatlas.med.jhmi.edu
Types of Insulin Onset (h) Peak (h) Effective Duration (h) Rapid Acting Insulin lispro (Humalog) <0.3-0.5 0.5-2.5 3-6.5 Insulin aspart (Novolog) <0.25 0.5-1.0 3-5 Insulin glulisine (Apidra) <0.25 1-1.5 3-5 Short Acting Regular (Humulin R or Novolin R) 0.5-1.0 2-3 3-6 Intermediate Acting NPH (Humulin N or Novolin N) 2-4 4-10 10-16 Long Acting Insulin glargine (Lantus) 2-4 flat 20-24 Insulin detemir (Levemir) 0.8-2 Dose Dependent (dose dependent) 12 hr for 0.2 U/kg 20 hr for 0.4u/kg, up to 24 hr (binds to albumin) Mixes Humulin/Novolin 70/30 (NPH/Regular) Humalog/Novolog 75/25 (Insulin lispro/aspart protamine/lispro/aspart)
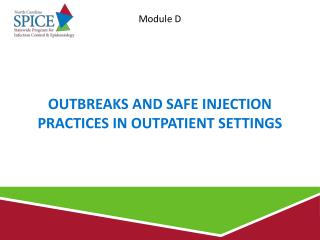
Pharmacokinetics of Various Insulin Insulin Analogues NEJM 2005: 352; 174-83
Blood Glucose Goals • Fasting Glucose: 70-130 • Pre-prandial goal: 70-130 • Postprandial goal: <180
Terminology • Basal Insulin: • Long acting insulin. Required in all type I patients, and patients over glycemic target. Required even when NPO • Prandial (Nutritional) Insulin: • Scheduled short acting insulin given in anticipation of carbohydrate induced hyperglycemic excursion • Adjust amount given if nutrition is diminished or interrupted • Correction Insulin: • Short acting insulin given in addition to scheduled insulin as a response to unexpected hyperglycemia. If this is used extensively, then scheduled insulin should be adjusted or added Subcutaneous Insulin Order Sets and Protocols: Effective Design and Implementation Strategies. Journal of Hospital Medicine: Vol 3, Issue 5, supplement 5 – S29-S41
Case I - Treatment • Initiate basal therapy with insulin glargine or NPH • Calculation of basal insulin: • Initiate with 0.2-0.4 units/kg and higher for patients with known insulin resistance • Would start with 0.3 units/kg, or more, in this patient with obesity and acanthosis • Weight: 110kg • 0.3 x 110 = 33 units, rounded to nearest even # = 34 units. • Written instructions to self-titrate dose by 2-4 units every 4 days for fasting glucoses > 130. • Would also suggest he stop at 60 units (0.5 units/kg). • Consider fast to evaluate basal dose • Add prandial insulin coverage, starting with largest meal
Management of Hyperglycemia in Type 2 Diabetes: A Consensus Algorithm for the Initiation and Adjustment of Therapy Diabetes Care 2006, Vol 29, number 8 1963-1972
Case II 32 yo overweight man with DM type II currently on Novolin 70/30 insulin, 30 units with breakfast and 20 units with dinner. Review of glucose log shows fasting glucoses around 200’s and pre-dinner glucoses (220’s), with frequent hypoglycemia occurring predominately before lunch, mainly on days that he eats a late lunch. He always eats a substantial bedtime snack due to a memorable episode of nighttime hypoglycemia. He has gained 10 pounds in last 3 months and is now 220 pounds. He wants to minimize number of insulin injections. What adjustments would you make?
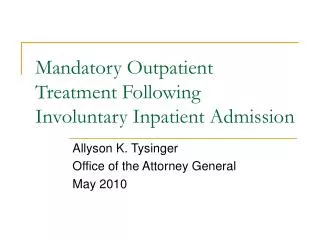
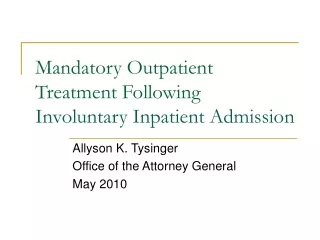
Mixed Insulin Regimens Diabetes Education Online – University of California San Francisco (www.deo.ucsf.edu/.../graph_sliding_premixed2.gif)
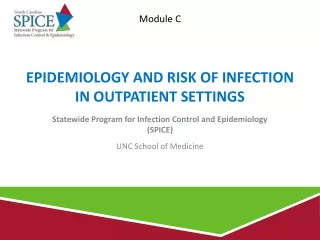
Case II - Treatment • Current regimen: • 30 units 70/30 in AM = 21 units N, 9 units R • 20 units 70/30 in PM = 14 units N, 6 units R • Calculation of total daily insulin dose: • 0.4 – 0.8 units x weight (kg), based on insulin sensitivity • Case II: 0.5 x 100 = 50 units/day • 50% as basal, 50% as bolus • Basal = 25, Bolus = 25 • Could change to: • NPH 18 units in AM mixed with Aspart 8 units AC breakfast • Additional NPH at breakfast will help cover lunchtime hyperglycemia • Aspart 10 units AC dinner (his biggest meal) • NPH 12 units HS
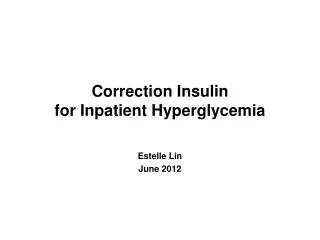
NPH and Rapid Acting Insulin NPH AM and AC dinner NPH AM and HS
Case III 24 yo man presented 3 days ago with DKA and was diagnosed with type I diabetes. He is currently on an insulin infusion. He has received 40 units of insulin over the last 24 hours (avg = 1.67 units/hr), is eating a regular diet, and is ready for transfer to the floor. Exam: Wt 176 lbs (80kg) How would you transition him to SC Insulin?
Case III • Calculation of Total Daily Dose (TDD) of Insulin • 1. Using Insulin Infusion Information • 80% of total dose: 0.8 x 40 = 32 units • Avg rate x 20: 1.67 x 20 = 32 units • May represent only basal amount if pt was NPO during infusion • 2. Calculation based on body weight • 0.4-0.6 units/kg for patients without significant insulin resistance: 0.4units/kg x 80kg = 32 units • Calculation of basal insulin: • 50% of TDD = 16 units or 0.2 units/kg x 32kg = 16 units • Be sure to give basal insulin at least 2 hours prior to stopping insulin infusion
Case III continued • Calculation of prandial insulin: 1. 50 % of TDD divided between 3 meals: 16 units – approximately 5 units/meal 2. Carbohydrate ratio: (“Rule of 500”) • 500/TDD of insulin = how many grams of CHO 1 unit of insulin will cover • Example: 500/32 units = 15.625 – round to 15 • One unit of meal-time insulin for every 15 grams of carbohydrates • Meals at MCV contain approx. 60 grams of CHO. For our patient, 4 units for each meal would be a starting point • Calculation of Correction Factor: (“Rule of 1500”) • 1500/ Total Daily Dose of Insulin = how many mg/dl 1 unit of insulin will lower blood sugar • Example: 1500/32units = 46.875 – rounded up 50 • One unit of insulin should lower glucose by 50 mg/dl • For glucose of 350, 4 units of Aspart should lower level to 150
Examples of Standardized Correction Doses ** Note that HS correction dose is significantly less and maybe zero ** Subcutaneous Insulin Order Sets and Protocols: Effective Design and Implementation Strategies. Journal of Hospital Medicine: Vol 3, Issue 5, supplement 5 – S29-S41
Case III -Continued • Patient does not like hospital food and eats varying amounts of meal. What you should do? • Patient is going to be made NPO for procedure. What should you do?
Case III - Continued • NPO status • If diabetic, especially type I, is to be NPO, be sure to continue basal insulin • Can decrease dose by 10% or 20% if uncertain of true basal needs • Change glucose monitoring to Q 6 hours • If patient’s appetite or PO intake is uncertain • Give mealtime Aspart after the meal • Can give ½ dose (2 units, for example) if about 50% of meal is eaten • If patient is able to count carbohydrates, he/she could tell nurse how much insulin to give after the meal, based on amount eaten
Case III Glucoses Insulin regimen Basal Insulin: Glargine 16 units QAM Prandial Insulin: Aspart 5 units AC meals Correction Factor: 1 unit/50 mg/dl above 150 Glucoses What adjustments would you make to insulin regimen?
Case IV 55 yo with DM type II, admitted with pneumonia. Meds: Glyburide 10mg daily Metformin 1 gram BID Exam: Wt 225 pounds (102 kg) Labs: Serum Glucose 285 Cr 1.5 (baseline of 1.2) Hgb A1c two months ago was 8.1 How would your manage his diabetes?
Hyperglycemia in the Hospital Management of Hyperglycemia in the Hospital Setting NEJM 335:18 Nov 2006
Inpatient Management of Diabetes • Every diabetic patient should have recent A1c to assess control on diabetic regimen. If unknown or not recent, order A1c on admit • If A1c is <8%, outpatient regimen can be considered. If on oral meds, will need to verify there are no contraindications (renal, liver, and cardiac function, other medications, procedures, nutritional status, etc) • If A1c is >8% will need basal insulin, if on oral meds. If on insulin, will need adjustments to prior insulin regimen • Order Accuchecks AC meals and HS. Q6 hours if NPO
Inpatient Management of Diabetes • Basal insulin: 0.2-0.4 units/kg in 2 divided doses for NPH. Glargine can be given in AM or bedtime • Prandial Insulin: MCV meals contain 60 g of CHO • Use “rule of 500” to calculate, or can start with between 4 (CHO 1:15) to 6 (CHO ratio of 1:10) units AC meals • Correction Dose: • Would at least provide correction for glucoses >300 • Aspart 6 units for glucoses >300 is reasonable for most patients • Use rule of 1500 to adjust. For example, if correction factor is 1:20 and glucose is 350, with target glucose of 150, the difference is 200. 200/20 = 10 units. 10 units of Aspart should lower glucose of 350 to 150 range
Case IV • Total Daily Dose (TDD) : 0.6 units/kg = 0.6 x 102 = 60 Units • Basal Insulin: 50% of TDD = 30 units or 0.3 units/kg x 102 = 30 • NPH 15 units AM and HS • Glargine 30 units • Prandial Insulin: A. 50 % of TDD = 30 units • Aspart 10 units AC meals B. Rule of 500 = 500/60 = 8.33. For 60g CHO/meal. 60/8.3 =7 • Aspart 7 units AC meals • Correction Dose: A. Aspart 6 units prn for glucose > 300. B. Rule of 1500: 1500/60 = 25. 1 U of insulin lowers glucose by 25
Case IV Correction Dose Glucose Insulin Glucose Insulin < 70 Assess patient, treat <70 Assess + treat 71-150 No additional insulin 70-150 None 151-175 1 unit 151-200 2 units 176-200 2 units 201-250 4 units 201-225 3 units 251-300 6 units 226-250 4 units 301-350 8 units 251-275 5 units 351-400 10 units 276-300 6 units 400 + 10 units + call 301-325 7 units 326-350 8 units 350-400 10 units 400+ 10 units and call MD
Case V 65 yo with DM type II and COPD admitted with COPD exacerbation. Home regimen was NPH 20 units AM, HS and Aspart 10 units AC breakfast and AC dinner. He is to be on prednisone 60mg daily as an inpatient and then will receive prednisone taper over 10 days on discharge Exam: Weight 80 kg How would you adjust his insulin regiment to account for hyperglycemic effects of corticosteroid?
Case V • Corticosteroids induce insulin resistance • Although prednisone is dosed every 24 hours, hyperglycemic effect is only a little over 12 hours • Once above 40mg, increasing doses of prednisone do not have added hyperglycemic effects • NPH’s has a duration of action to cover this effect • NPH 0.1 units/kg for every 10mg of prednisone up to 40 mg
Case V For our 80 kg patient: Dose of prednisoneNPH to be added home regimen 60mg 0.4 U/kg x 80kg = 32 units 40mg 0.4 U/kg x 80kg = 32 units 20mg 0.2 U/kg x 80kg = 16 units 10mg 0.1 U/kg x 80 kg = 8 units For 60 mg of prednisone, he would take 20 U NPH + 32 U NPH = 52 U NPH in AM at the same time as prednisone He will continue 20 U NPH at bedtime and same mealtime Aspart insulin He may likely need more dinner Aspart while on prednisone
Case VI 60 yo with DM type II, laryngeal cancer, s/p surgery. He is currently on continuous TFs with Two Cal HN at 60 ml per hour. He is unsure of his home diabetes regimen. Exam: Weight 85 kg Labs: Hgb A1c is 8.4 How would you control his glucoses while on the TFs?
Case VI 1. Calculate Total Daily Dose of Insulin 0.6 x 85 kg = 51 Units (50 units) 2. Calculate basal needs: 0.3 units/kg x 85 = 25.5 units (25 units) 2. Rule of 500 to calculate carbohydrate ratio 500/50 = 10 1 unit will cover 10g of carbohydrates 3. Calculate total grams of carbohydrates to be covered -1st calculate total amount (volume) of TFs 60 ml/hr x 24 hours = 1440 ml/day -Next calculate how many grams of carbohydrates (CHO) this gives/day Two cal HN has 52 g of CHO per 8 fl oz can (236ml) or 0.22 g CHO/ml 0.22 g CHO/ml x 1440 ml/day = 317 g CHO/day -Finally calculate how much insulin is needed to cover CHO content of TFs 317 g CHO/day x 1U/10g CHO = 31.7 or 32 units 4. Basal insulin + Insulin to cover TFs = 25 U + 32 U = 57 Units
Case IV • Options for TF coverage: • Glargine daily, Regular every 6 hr, Aspart every 4 hr, or NPH every 8 hr • Tube feeds tend to be interrupted often (i.e. for procedures or because the patients pull them out) • For our patient, we would choose NPH every 8 hours • 57 units total/ 3 = 19 units NPH Q 8 hours • *If TFs are stopped, he will need D10 infusion to cover NPH
Key Points • Individualize insulin therapy based on • Etiology of diabetes • Weight, BMI and anticipated insulin resistance • Clinical setting- inpatient vs outpatient • Patient’s diet or nutritional status • Treatment goals
The End Any Questions?