Download
1 / 14
140 likes | 366 Views
Recovery from an Osteoporotic Hip Fracture. Nicholas Wayne Sheets. Purpose. Discuss the affects of experiencing an osteoporotic hip fracture Review the three principles of Mind, Consciousness, and Thought

E N D
Recovery from an Osteoporotic Hip Fracture Nicholas Wayne Sheets
Purpose Discuss the affects of experiencing an osteoporotic hip fracture Review the three principles of Mind, Consciousness, and Thought Examine how the three principles can be presented to a patient who has experienced an osteoporotic hip fracture
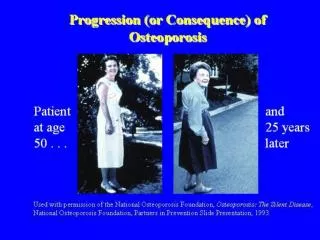
Osteoporosis Weakening of the bones Affects primarily elderly populations Results in fractures
Osteoporosis • Pain • Disability • Medical Bills • Depression • Patients experience increased depression after a hip fracture • Mortality • Patients who experience a hip fracture are 50% more likely to die in the following year
Resiliency Teach patients the 3 principles of Mind, Consciousness, and Thought Help patients recognize how their own thinking affects their health Hope patients experience insights
Teaching • Health Care Providers • A patient spends 6-7 days in a hospital after experiencing an osteoporotic hip fracture
3 Principles Mind, Consciousness, & Thought Taking complexity and simplifying Are discovered and not created
Mind Formless Gives rise to the following principles of consciousness and thought Given many different names such as spirit, God, or Allah
Consciousness • Gives us the ability to experience thought • (Our consciousness follows our thought) • Higher level of consciousness • The elevator metaphor
Thought Our thoughts are constantly occurring and we are always aware of them Thought + Consciousness = Personal Reality We can recognize how our moods affect our thoughts
Conclusion • The three principles can help patients experience better outcomes • Though the principles are simple, simply being knowledgeable does not allow full benefits • Strive to experience insights
End nsheets1@mix.wvu.edu
Reference Banks, S. (2001). The enlightened gardener. Vancouver, Canada: Lone Pine Publishing. Beaupre, L.A., et al. (2005). Does standardized rehabilitation and discharge planning improve functional recovery in elderly patients with hip fracture? Archives of Physical Medicine and Rehabilitation, 86(12), 2231-2239. Bellizzi, K.M., & Blank, T.O. (2007). Cancer-related identity and positive affect in survivors of prostate cancer. Journal of Cancer Survivorship: Research and Practice, 1(1): 44-88. Boonen, S., & Singer, A.J. (2008). Osteoporosis management: impact of fracture type on cost and quality of life in patients at risk for fracture. Current Medical Research and Opinion, 24(6), 1781-1788. Gehlbach, S.H., Avrunin, J.S., & Puleo, E. (2007). Trends in hospital care for hip fractures. Osteoporosis International, 18(5), 585-591. Givens, J.L., Sanft, T.B., & Marcantonio, E.R. (2008). Functional recovery after hip fracture: the combined effects of depressive symptoms, cognitive impairment, and delirium. Journal of the American Geriatrics Society, 56(6), 1075-1079. Kanis, J.A., et al. (2004). A meta-analysis of previous fracture and subsequent fracture risk. Bone, 35(2), 375-382. Koenig, H.G. (2000). MSJAMA: religion, spirituality, and medicine: applications to clinical practice. The Journal of the American Medical Association, 284(13), 1708.
Reference Kosmin, B.A., Mayer, E., & Keysar, A. (2001). American religious identification survey. Retrieved July 26, 2008, from The Graduate Center of the City University of New York. Web site: http://www.gc.cuny.edu/faculty/research_briefs/aris.pdf Mezuk, B., Eaton, W.W., & Golden, S.H. (2008). Depression and osteoporosis: epidemiology and potential mediating pathways. Osteoporosis International, 19(1), 1-12. Oakley, R. (2004). How the mind hurts and heals the body. American Psychologist, 59(1), 29-40. Paksima, N., et al. (2008). Predictors of mortality after hip fracture: a 10-year prospective study. Bulletin of the NYU Hospital for Joint Diseases, 66(2), 111-117. Pransky, J. (2003). Prevention from the inside-out. Bloomington, IN: Authorhouse. Salkeld, G., et al. (2000). Quality of life related to fear of falling and hip fracture in older women: a time trade off study. British Medical Journal, 320(7231), 341-346. Sedgeman, J.A. (2003). Principles underlying life experiences: the beauty of simplicity. Morgantown, WV: Sydney Banks Instituted of Innate Health, West Virginia University School of Medicine. Silverman, S.L., Shen, W., Minshall, M.E., Xie, S., & Moses, K.H. (2007). Prevalence of depressive symptoms in postmenopausal women with low bone mineral density and/or prevalent vertebral fracture: results from the Multiple Outcomes of Raloxifene Evaluation (MORE) study. The Journal of Rheumatology, 34(1), 140-144. Williams, M.A., Oberst, M.T., & Bjorklund, B.C. (1994). Post hospital convalescence in older women with hip fracture. Orthopaedic nursing / National Association of Orthopaedic Nurses, 13(4), 55-64.