Download
1 / 18
180 likes | 621 Views
Histoplasma Capsulatum. Thin walled oval yeastDimorphic: Filamentous in environment.Yeast in tissue.. Epidemiology: . Endemic to OHIO and MISSISSIPPI RIVER Valleys.Found in organic soil.Bat, Chicken and Bird excrement.. Epidemiology contd

E N D
1. Disseminated Histoplasmosis (DH). Soham Puvvada, MD.
2. Histoplasma Capsulatum Thin walled oval yeast
Dimorphic:
Filamentous in environment.
Yeast in tissue.
3. Epidemiology:
4. Epidemiology contd�
5. Pathogenesis Inhalation of mycelial filaments.
When mycelia(microconidia) reach alveoli, converted to yeast form.
Activate PMN, macrophages, lymphocytes, NK cells.
Phagocytized by macrophages in an attempt to clear infection.
6. Failure to activate macrophage fungicidal capacity seems to be key immune defect in progressive DH
Study based on murine model: exogenous IL2 increased IFN-gamma, TNF-alpha, decreased colony counts and increased survival(Zhou et al, Infect Immun 1997).
Hematogenous and lymphatic spread via macrophages to adjacent lymphatic nodes, liver, spleen, lymph nodes, adrenal glands, bone marrow.
Data from autopsy studies suggests also involvement of gi tract, of those undergoing exam of brain, meninges, 2/3 demonstrate cns involvement. �however with autopsy studies bias towards severe end of spectrum of dis, tissues less commonly involved in milder cases, histopathologically perivasculits with necrosis with more severe involvement of the meninges, adrenal glands.Data from autopsy studies suggests also involvement of gi tract, of those undergoing exam of brain, meninges, 2/3 demonstrate cns involvement. �however with autopsy studies bias towards severe end of spectrum of dis, tissues less commonly involved in milder cases, histopathologically perivasculits with necrosis with more severe involvement of the meninges, adrenal glands.
7. Pathology Diffuse histiocytosis, Focal histiocytosis & Tuberculoid granulomas.
Histiocytosis refers to macrophage infiltration in affected tissues.
Granulomas less common in DH, & usually seen in pts with lower fungal burdens, and more intact immune function: Inflammatory reaction at the site of infection with caseating or noncaseating granuloma formation. Yeast may remain viable in granulomas for an extended period of time. Three types of tissue response have been described in disseminated histoplasmThree types of tissue response have been described in disseminated histoplasm
8. Risk factors AIDS:
most common endemic mycoses in pts with AIDS.
First case described in 1982.
AIDS defining illness per CDC in 1987.
US:2-5% of HIV positive population.
Usually disseminated progressive, as opposed to other clinical syndromes.-median cd4 count=50.
Usually vague antecedent c/o of fever, wt loss malaise, over weeks, vague resp symptoms.
Decreased incidence since HAART.
9. Extremes of age
Transplant Recipients:
exogenous infection from conidia or reactivation of quiescent disease.
Also can be transmitted from donor.
Immunosuppressive meds: Steroids, TNF-Alpha inhibitor therapies, Methotrexate.
10. Clinical Syndromes of Histoplasmosis.
Acute Primary Histoplasmosis
Chronic Pulmonary Histoplasmosis
Mediastinal Granulomatosis
Fibrosing Mediastinitis
Disseminated Histoplasmosis
11. Clinical Presentation of DH: Fever, hepatosplenomegaly, generalized LAD.
DH Septicemia is a well-described entity:
Hypotension, ARDS, hepatic, renal failure, DIC.
Usually later in the course of DH-occur in pts who did not seek attention early: 13% of AIDS pt with histo*(1990 study).
Skin: papules to ulcers to E.multiforme
GI: 10% of cases, diarrhea, vague, abdominal pain. May have GI bleeding, polypoid, ulcerative lesions in colon.
Neuro: AMS with focal neurologic findings(10-30%), encephalopathy, lymphocytic meningitis, focal parenchymal lesions in brain/SC. Historically, worse prognosis.
Skin findings proteanSkin findings protean
12. Adrenal Insufficiency: well recognized in DH. If not diagnosed correctly, fatal outcomes despite appropriate antifungal therapy.
Rarer Manifestations:
Pleuritis
Pericarditis
Pancreatitis
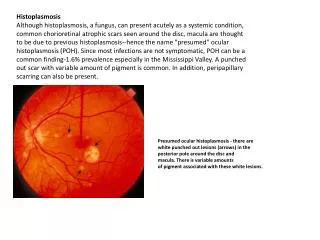
Chorioretinitis
Endocarditis
Thrombotic microangiopathy
Hemophagocytic syndrome**
13. Diagnostic Testing: LAB Findings:
Leukopenia, anemia, thrombocytopenia suggestive of marrow infiltration.
Markedly elevated LDH seen in pts with AIDS(Corcoran et al, Clin Inf Dis 97), as well as ferretin levels>10000 (Kirn, AIDS 1995).
Occasionally seen on a peripheral smear.
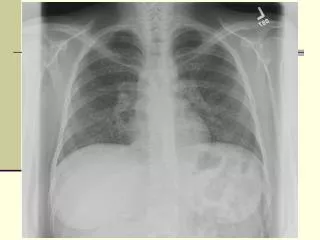
RADIOLOGY:
severe immunosuppression, rarely causes focal infiltrates. Usually diffuse interstitial or reticulonodular patterns. Often resembles PCP or miliary TB.
Less immunosup: mediastinal LAD, nodular opacities, sometimes normal CXR.
14. Antigen Detection: Urine: most sensitive rapid assay-upto 95% sensitivity in DH and AIDS, false + seen with blastomycoses, coccidiomycoses, paracoccidiomycoses.
Serum: -upto 85 % sens in AIDS, false+ in approx 16% of solid transplant pts that received Rabbit ATG.
Also from CSF, BAL.
15. Serologic Testing: Immunodiffusion and complement fixation methods.
In pts with intact immune systems, Ab develop at high levels with 4-6 weeks.
Rarely, provide diagnosis in AIDS because in severe immunosuppression and DH, false negatives even in active infection.
16. Culture: Gold standard for diagnosis, but isolation takes upto 4 weeks and therefore impractical as a criterion for treatment initiation.
In AIDS pt with DH, studies have shown 91 % sensitivity in isolation from peripheral blood cultures and upwards of 90% sensitivity in isolation from bone marrow specimens.
17. Treatment Options: Induction Phase:
Directed at controlling clinical manifestations of disease.
Duration 12 weeks.
Moderate to Severe Infection: Ampho B 0.7-1mg/kg IV qd or Ambisome 3-5 mg/kg IV qd- once clinically improved may transition to itraconazole.
Mild Infection: Itraconazole 300 mg po or IV bid for 3 days, then 200 mg po bid, serum level>2ug/ml.
18. Maintenance Therapy: to prevent relapse.
Prior to HAART, upto 80% relapse rates therefore often lifelong therapy recommended. Currently, for patients with sustained improvement of HAART, 12 months of total antifungal therapy. Usually with Itraconazole 200-400 mg po q day.
Other agents:
ketoconazole �high relapse rates.
Caspofungin does not have adequate activity.
Voriconazole less tolerated than Itra, therefore not used for routine treatment; however can achieve reasonable CSF concentrations.
Posaconazole highly effective at reducing fungal burden and equally effective as Ampho. In one open label trial-7 pts, who received posaconazole as salvage therapy after failing Ampho, 6 had successful outcomes including 1 case of DH related meningitis.
19. References: