Download
1 / 34
690 likes | 3.3k Views
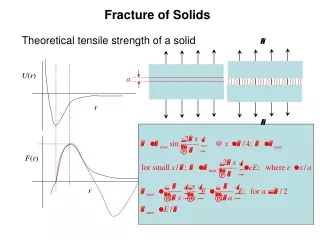
Fracture of tibia. . Proximal tibial fracture. Mechanism of injury : - Due to valgus or varus force with axial loading Causes : - 52% - due to bumper injuries 17% - due to fall from heights. 31 % - miscellaneous causes Types :-

E N D
Proximal tibial fracture Mechanism of injury : - • Due to valgus or varus force with axial loading Causes : - • 52% - due to bumper injuries • 17% - due to fall from heights. • 31 % - miscellaneous causes Types :- 1. Articular (Hohl and Moore`s classification ) Plateau fracture fracture dislocation 2. Nonarticular
Hohl & Moore’s classification • Fracture dislocations1. Split fracture 2. Entire condyle fracture3. Rim avulsion fracture ( Involves lateral condyle, associated with capsular tears and vascular injuries )4. Rim compression type (Unstable associated with avulsion of cruciates)5. Four part fracture (Unstable with Collateral avulsed And neurovascular injuries)
Plateau fracture split compression Minimally displaced Local compression Total condylar depression Bicondylar fracture
Schatzker classification I: Lateral split II: Lateral split with depression III: Pure lateral depression; no splitting IV: Medial tibial plateau split or split depression type fracture V: Split fractures of both medial and lateral tibial plateaus VI: Split extends to metadiaphysis, separating metaphysis from diaphysis - Types I to III are low-energy injuries. - Types IV to VI are high-energy injuries. - Type I usually occurs in younger individuals and is associated with medial collateral ligament injuries - Type III usually occurs in older individuals
Schatzker 1: Split Fracture of the lateral side.
Schatzker 2: Lateral split with depression
Schatzker 3: • . Pure lateral depression; no splitting
Schatzker 4 . Medial tibial plateau split or split depression type fracture
Schatzker 5: Split fractures of both medial and lateral tibial plateaus
Schatzker 6 Split extends to metadiaphysis, separating metaphysis from diaphysis
Clinical features • Pain • Swelling • Deformity • Haemarthrosis • Decrease movement of knee • Instability in valgus or varus
Investigations Routine : - • AP and lateral view (to demonstrate majority of tibial condyle fractures ) • Oblique view ( to localise the fracture) • CT scan (study the depth of depression )
Schatzker I: • Definition:. Lateral split • Etiology: Often due to valgus stress. Occurs in younger patients with stronger bones, which are resistant to depression. Often due to a bumper injury. • Common associated injuries: Lateral meniscal tear. The lateral meniscus may also become entrapped in the fracture and require arthroscopy. • Treatment: Typically, lateral fixation.
Schatzker II • Most common tibial plateau fracture. • Definition: Lateral split with depression. • Etiology: Often due to valgus or axial stress. Occurs in older patients with osteoporosis with bones that do not resist depression. • Common associated injuries: Lateral meniscus, medial meniscus, and medial collateral ligament. • Treatment: Typically, lateral fixation. The depressed fragments are elevated and supported with bone graft.
Schatzker III: • Definition: Pure lateral depression; no splitting • Etiology: Older patients with osteoporosis. Often just due to a fall. • Common associated injuries: If the depressed fragments are lateral and posterior, it is associated with joint instability. • Treatment: If there is instability, the fractured fragments are elevated and supported with bone graft and lateral internal fixation.
Schatzker IV: • Definition: Medial tibial plateau fracture that may be a split or split depression type fracture. • Etiology: Varus stress. Often severe trauma. • Common associated injuries: Associated with avulsion of the intercondylar eminence, which may indicate anterior cruciate ligament injury. Lateral collateral ligament injury. Peroneal nerve injury. Popliteal artery injury. • Treatment: Medial plate and screws.
Schatzker V: • Definition: Split medial and lateral tibial plateau (Bicondylar). Metaphysis is still in continuity with the diaphysis. • Etiology: Often pure axial stress with severe trauma. • Common associated injuries: Neurovascular, ACL, and meniscal injuries. • Treatment: Typically, medial and lateral internal fixation. • .
Schatzker VI: • Definition: Metaphyseal fracture that separates the articular surface from the diaphysis. • Etiology: High-energy trauma. • Common associated injuries: Neurovascular injury and compartment syndrome. Also meniscal, ACL, and collateral ligament injuries. • Treatment: Typically medial and lateral internal fixation
Treatment In plateau fracture Undisplaced fractures : - above knee , POP cast with 5 degree flexion or cast bracing Displaced fractures : - closed reduction , with or without skeletal tractionand a long leg cast In depressed fractures : - • For less than 8 mm depression (above knee casts ) • For more than 8 mm with a large splint fragment, skeletal traction • For more than 8 mm with a smaller splint fragment (ORIF with bone grafting after elevation of the depression )
Cont.. In splint fracture:- • ORIF • Skeletal traction ( comminuted fractures )
Malunion or nonunion: This is most common in Schatzker VI fractures at the metaphyseal-diaphyseal junction, related to comminution, unstable fixation, implant failure, or infection. Posttraumatic osteoarthritis: This may result from residual articular incongruity, chondral damage at the time of injury, or malalignment of the mechanical axis. Peroneal nerve injury: This is most common with trauma to the lateral aspect of the leg where the peroneal nerve courses in proximity to the fibular head and lateral tibial plateau. Popliteal artery laceration. Avascular necrosis of small articular fragments: This may result in loose bodies within the knee. COMPLICATIONS • Knee stiffness • Infection • Compartment syndrome • Malunion or nonunion • Posttraumatic osteoarthritis • Peroneal nerve injury • Popliteal artery laceration. • Avascular necrosis
Distal tibia fractures PILON FRACTURES ( TIBIAL PLAFOND FRACTURES ) - Due to axial loading forces following the RTA or fall from height - males are more commonly affected than females - mean age is 35 to 40 years
Classification • Type 1 : - undisplaced cleavage fracture of the joint and are usually low energy injuries in which the fracture fragments are nearly aligned • Type 2 : - displaced but minimally comminuted fractures and are usually moderate energy injuries • Type 3 : - highly comminuted and displaced fractures and are usually high energy injuries
Type 1 : - undisplaced cleavage fracture of the joint and are usually low energy injuries in which the fracture fragments are nearly aligned
Type 2 : - displaced but minimally comminuted fractures and are usually moderate energy injuries
Type 3 : - highly comminuted and displaced fractures and are usually high energy injuries
Clinical features • Pain • Swelling • Deformity • Inability to bear weight • Loss of sensation
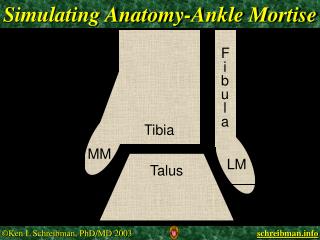
Findings • Look for peripheral pulses and the sensation in the foot • look for deformity and swelling • Look for local bruising , fracture blisters and if there is a tense calf muscles (indicates compartmental syndrome ) • Investigations • X – rays AP , lateral and ankle mortise view • CT scan (nature and extent of the injury )
Treatment Minimally displaced fractures :- treated with a plaster cast on external fixator Displaced fractures : - open reduction and internal fixation with plate and screws
Complications include . infection • mal-union or union of the fracture in a unacceptable position • non-union that is failure of the fracture to unite • arthritis of the ankle joint