Download
1 / 30
300 likes | 327 Views
This article discusses the Sverdlovsk anthrax incident and recent cases of bioterrorism-related anthrax outbreaks. It provides information on the symptoms, diagnosis, and treatment of inhalational anthrax. The article also includes illustrations and timelines of the cases.

E N D
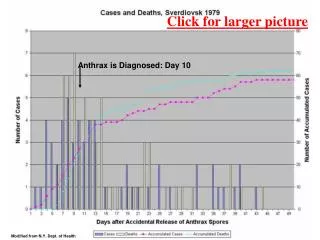
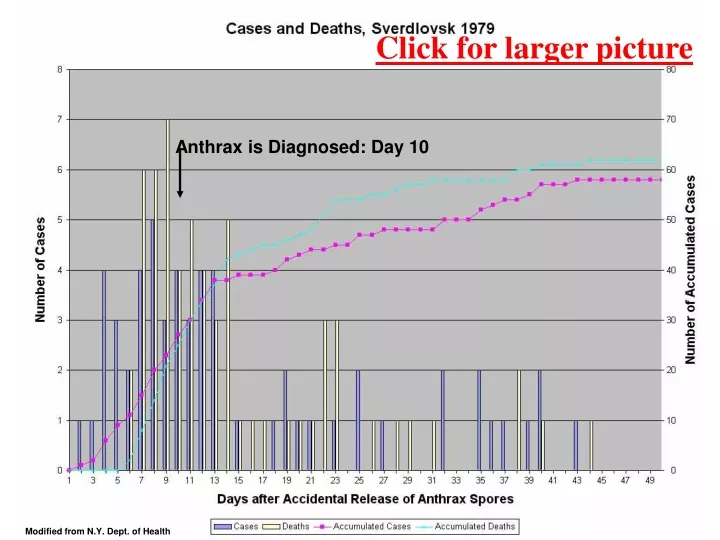
Anthrax is Diagnosed: Day 10 Click for larger picture Modified from N.Y. Dept. of Health
Anthrax as a Biological Weapon (JAMA. 1999;281:1735-1745) Figure 4. Day of Onset of Inhalational Anthrax Following Sverdlovsk AccidentFigure is based on data from Guillermin.68
Anthrax is Diagnosed: Day 10 Click for larger picture This curve approximates that of the accumulated deaths more closely (JAMA. 1999;281:1735-1745)
Lidia Tretyakova looks at the tombstone of her father, Lazar Karsayev, at a cemetery in Yekaterinburg, Russia, Thursday, Oct. 18, 2001. A mysterious outbreak of anthrax killed at least 68 people, including Karsayev, 22 years ago in the Russian industrial center of Sverdlovsk, today known as Yekaterinburg. At the time, neither the victims nor their families suspected they had been hit by a biological weapon.
Laboratory workers at the Sverdlovsk regional epedemiological service put on the special suits they wear when working with anthrax and other dangerous bacteria in Yekaterinburg, Russia, Wednesday, Oct. 17, 2001
A general view of the Stepnogorsk Scientific Experimental and Production Base (SEPB) in Stepnogorsk, 220 km (100 miles) northwest of Kazakstan's new capital of Astana, Monday, Oct. 22, 2001. The SEPB was the biggest anthrax-manufacturing plant in the world. (AP Photo)
Scientists work in an environmental monitoring laboratory of Stepnogorsk Scientific Experimental and Production Base (SEPB) in Stepnogorsk, 220 km ( 100 miles) northwest of Kazakstan's new capital of Astana, Monday, Oct. 22, 2001. The SEPB was the biggest anthrax-manufacturing plant in the world. (AP Photo)
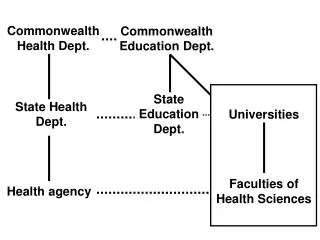
Review of some Consensus guidelines J.A.M.A.1979. 281: 1735-1745. Working Group on Civilian Biodefense
Click for larger picture J.A.M.A.1979. 281: 1735-1745. Working Group on Civilian Biodefense
Click for larger picture J.A.M.A.1979. 281: 1735-1745. Working Group on Civilian Biodefense Ratified in MMWR. 2001. 50: 889-897. (Oct. 19, 2001)
The recent Anthrax victims The victims of the recent terrorist use of anthrax bacilli started to appear in October 2001. On October 2 the spinal fluid of a patient in Miami showed large Gram positive bacilli, confirmed on October 4 as Bacillus anthracis
Inhalational Patients Recovered Died Ottilie Lundgren, 94 Inhaled Connecticut farm Died, Nov.21, 2001 List of recent bioterrorism-related Anthrax victims Norma Wallace, 56
More illustrations Click for larger picture Data mostly from Jernigan et al., Emerging Infectious Diseases, 7: 933-944, 2001 Patient No. 11 is not presented in the Jernigan series; the data appeared in the news.
Timeline of 10 cases of inhalational anthrax in relation to onset of symptoms, October through November 2001 Click for larger picture Jernigan et al., Emerging Infectious Diseases, 7: 933-944, 2001
Table 2, Jernigan et al., 2001. Emerging Infectious Diseases, 7: 933-944.
Click for larger picture Table 3, Jernigan et al., 2001. Emerging Infectious Diseases, 7: 933-944.
Gram stain, cerebrospinal fluid, Case 1 Clear diagnosis, Oct. 2, 2001
Chest X-ray, Case 2 – Diffuse consolidation, consistent with pneumonia of left lung No mediastinal widening
Computed tomography of chest, Case 2 Bilateral pulmonary consolidation and pleural effusioins
Chest X-ray, Case 7 – Mediastinal widening, left pleural effusion
Chest computed tomography, Case 7 – Mediastinal adenopathy, bilateral pleural effusions