Download
1 / 30
320 likes | 396 Views
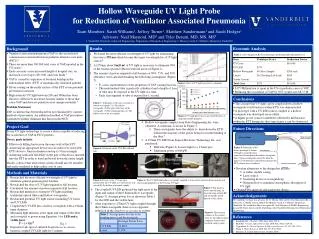
This study focuses on reducing Ventilator-Associated Pneumonia (VAP) in a medical ICU through a comprehensive approach, including education, interventions, and audits. Results show a significant decrease in VAP rates and substantial cost savings. The sustainable strategies implemented foster a culture of continuous improvement and enhanced patient care.

E N D
Ventilator Associated PneumoniaReduction in a Medical ICU Bela Patel, MD Tammy Campos, RN, MSN Ruth Siska, RN Bela Patel MD Tammy Campos RN Ruth Siska RN
“Nosocomial” Infections • Nosocomial Infections • Not present or incubating upon admission to the hospital (48hr rule) • Preferred: Hospital Acquired Infections (HAIs) • 5-10% of patients admitted to hospital or 2 million patients • 88,000 deaths per year • Costs exceed 4.5 billion/year • 1 outbreak per 10,000 discharges
On the horizon for us • Texas reporting • Law passed requiring mandatory reporting of HAI to TDSHS starting 2008 • Rates will be publicly available • Federal reporting • Bill introduced requiring mandatory reporting to CDC through NHSN • New national guidelines on infection control 2008 • Medicare • SCIP as core measure • Lower rate reimbursement for patients with HAI starting 2008
VAP • Leading cause of death amongst hospital-acquired infections • Mortality 46% compared to 32% percent for ventilated patients who do not develop VAP • Increased ventilator days • Increased ICU LOS
VAP defined • Patients mechanically ventilated for greater than 48 hours • Exhibit at least 3 or 5 following symptoms: • Fever • Leukocytosis • Change in sputum (color and/or amount), • Radiographic evidence of new infiltrates • Worsening oxygen requirements CDC 2003
Cost of VAP at MHH Cocanour, et al. Surgical Infections 2005.
VAP prevention “Vent Bundle” • Suctioning • Head of bed > 30o • Oral care • “Sedation holiday”
Memorial Hermann -MICU • 16 bed unit admitting 1100 patients per year • 60% ventilated >3 days putting them at greater risk for VAP • Chief diagnoses include septicemia, respiratory failure, HIV/AIDS, renal failure, and multisystem organ failure secondary to multiple co-morbid conditions • Previous improvement work had made respectable reductions in VAPs from 2-3 per month to <10 per year, however it was felt more was achievable
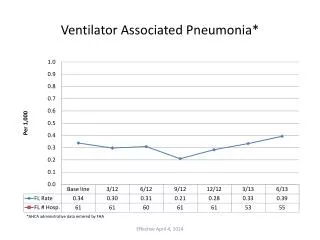
Aim and Measures Aim To reduce VAPs in the MICU to Zero within six months. Measures • Reduction in number of VAPs per 1000 ventilator days • Increased compliance with all aspects of the ventilator bundle.
Interventions: Education • MICU “Huddles” on VAP and mortality • Posted rates in the unit for staff and MDs to see • Posted rates in public areas for patients and family members to see • Reviewed bundle compliance regularly in multidisciplinary team meetings • Reviewed compliance and VAP rates at local and system critical care committees
Interventions: Implementation • Developed physician Rounding Tool to address VAP bundles • Appointed unit champions to assure patients were out of bed on daily basis • Formalize oral care process using chlorahexadine • Trained Patient Care Assistants (PCAs) in oral care • Mandated that oral care be a shared responsibility by RNs, Respiratory Therapists and PCAs increasing oral care from 4 times per day to 10 times per day • Computerized reminder alert for the care team • Located all oral care supplies near ventilators • Located isolation supplies –gowns, gloves, masks at entrance to every patient room
Interventions: Implementation • Increased isolation practices for all infected patients to include booties, head coverings • Implemented glycemic protocol to keep glucose between 80 and 150 • Implemented automatic insulin drip for all patients who had 2 consecutive finger sticks above 150 • Implemented standardized sedation protocol • Improved Sedation holiday practices by team approach to assessment • Improved transportation practices
Interventions: Audits • Implemented daily manager rounds to assure bundle compliance • Assured compliance with unit protocols by PRN staff and consulting MDs • Implemented a mini-RCA process for all VAPs to detect specific patient characteristics and system risk factors • Infectious Disease Dept conducts random weekly audits for bundle compliance • Infectious Disease Dept reviews all cases to diagnose VAPs based on CDC criteria
More to do: FMEA • Aspiration during transport • Cuff leaks • Unplanned extubations requiring reintubation
Results: Overall • VAP rate went from 8-12 per year to zero within three months. • No VAPs have occurred in the MHH-TMC MICU for 26 consecutive months • Compliance with all aspects of the VAP bundle is between 98 - 100%.
Results: Cost Savings • A financial analysis completed by our infectious disease and financial departments concluded that a VAP in any of our ICUs adds $57,000 in additional costs for additional antibiotics, ventilator time and ICU stay. • Cost avoidance for this project based on avoiding 8 VAPs per year is $456,000.
Sustainability • Takes a Village to raise a “Zero” • Culture Changed • Goal became Expectation • Work flow changes became routine • Reporting of “near misses” • Created a highly functioning multidiciplinary team
Conclusions and Next Steps • With concerted and focused effort “zero” is possible as an outcome. • As with any major improvement, the challenge is to maintain this level of performance. • Build on this methodology to achieve similar improvements for other hospital acquired infections in the Intensive Care Units.
Acknowlegements • UT Divisions of Critical Care, Pulmonary and Sleep Medicine • MHH ICU Nursing Staff • MHH Respiratory Therapy • MHH Nutrition Support • UT-MHH Academy of Patient Safety & Effectiveness