Download
1 / 36
360 likes | 384 Views
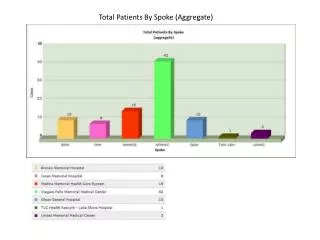
This study examines the effects of knowledge on the attitude and practice of diabetic and hypertensive patients at a railway health unit. The study involves a total of 175 patients, with insights on sources of information, lifestyle factors, and recommendations for improving care and awareness.

E N D
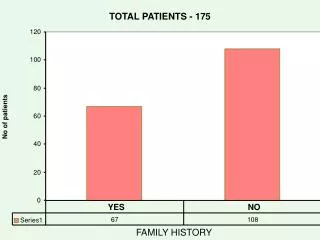
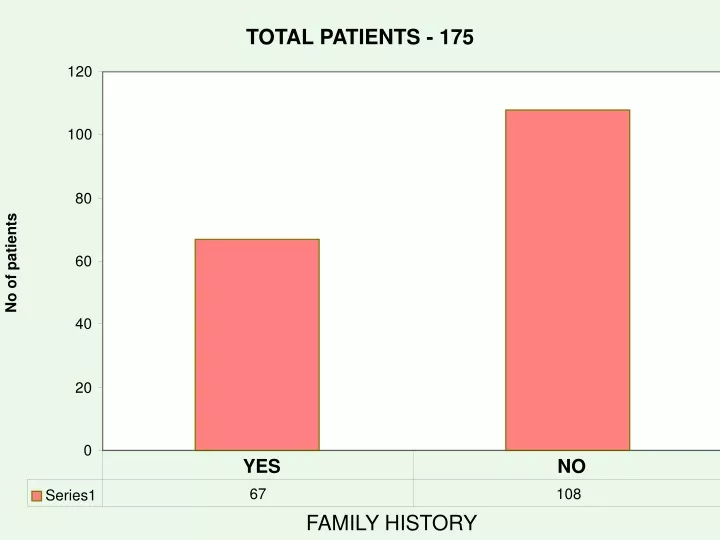
TOTAL PATIENTS - 175 120 100 80 No of patients 60 40 20 0 YES NO 67 108 Series1 FAMILY HISTORY
HYPERTENSION & DIABETES 160 140 120 100 No of patients 80 60 40 20 0 Railway hospital Private Regular treatment Irregular treatm 149 26 127 48 Series1 TREATMENT
Classification of patient 100 91 90 80 70 60 50 40 33 33 30 20 15 10 2 1 0 CLASS-1 CLASS-2 CLASS-4 RTD.EMPLOYEE CLASS-3 DEPENTANTS category
20 19 COMPLICATION 18 16 14 12 10 8 7 6 6 4 3 2 1 1 0 1 AMPUTATION RETINOPATHY NEPHROPATHY HEART ATTACK STOKE NON-HEALING ULCER
BODY MASS INDEX 115 120 100 80 49 60 40 6 5 20 0 > 17-< 27 < 17 > 27- < 32 > 32 5 115 49 6 Series1
WAIST-HIP RATIO: • How to Calculate Waist-Hip Ratio • Waist Hip Ratio is calculated by dividing your waist measurement by your hip measurement. Using a tape measure, measure your waist below your rib-cage but above your belly button. Then measure your hips - the widest part of your butt. Finally, divide your waist measurement by your hip measurement. • Ideally, women should have a waist-to-hip ratio of 0.8 or less. • Ideally, men should have a waist-to-hip ratio of 0.95 or less
REGULAR CHECK UP AT RH/PER NO 33% YES 67% YES NO
SOURCE OF INFORMATION SOURCE OF INFORMATION 3% 5% 4% 88% RADIO/TV NEWSPAPER MEDICAL STAFF FRIENDS
KNOWLEDGE KNOWLEDGE 160 YES-136 140 120 YES-102 NO-101 YES-96 100 NO-93 NO-91 YES-84 YES-82 NO-79 80 YES-74 NO-73 60 NO-39 40 20 0 WHAT IS HT? SYMPTOMS OF DM COMPLICA-TION OF DM SYMPTOMS OF HT COMPLICA-TION OF HT WHAT IS DM?
PRACTICE 160 NO-141 140 NO-125 120 NO-113 NO-105 100 NO-91 YES-84 80 YES-70 YES-62 60 YES-50 40 YES-35 20 HEALTHY/ BALANCED DIET 0 REGUL WEIGHT CHECK UP REGULAR EXECISE REGULAR BP CHECK UP BLOOD, URINE SUGAR CHECK UP
DISCUSSION: This study was conducted to gauge the effects of knowledge on the attitude-followed by practice among diabetic and HT patients, attending Railway health unit, Tondiarpet Marshaling Yard. Total patients for K.A.P study were 175. 68 of them were suffering from HT, followed by 66 with DM alone and 41 patients with DM and HT. 114 male patients and 61 female patients were included in this study. Most of the patients age ranged from 51-60 years (78), followed by 41- 50 years (73), > 60 years (16), and 30 – 40 years (8).
The most common source of information on diabetes was from medical staffs (80 T0 85%). This could be due to the fact that all newly diagnosed diabetic and HT patients are thoroughly briefed on diabetes by the doctors and the medical assistants. The respondents were tested on 6 aspects of knowledge on diabetes - what they understand by the disease, symptoms, complications, prevention, diet and exercise. 50% to 60% of the total 175 patients are having the adequate knowledge about HT and DM. 30% to 40% of the patients are having the attitude to control DM and HT.
80% to 85% of the patients collected the source of information about DM and HT from the Medical Department. Random blood sugar of 60% to 65% of diabetic patients was above 200 mgms. Only 3 Diabetic patients were periodically monitored by Hba1c level in blood from private laboratory. 95% of the total patients are Non-Vegetarian. 58% of the male patients are alcoholic, and 26% Male patients are smokers. 49/175 patients are over weight and 6/175 patients are Obese. Only 85% of the patients were not done lipid profile and 45% of the patients were monitored by eye check-up. 48% of the patients preferred private lab for their routine investigation for follow-up as their residence far away.
Conclusion: In many cases, we can prevent or treat these diseases, but in order to do so, we need to persuade people to make changes in diet, physical activity, and their own awareness and monitoring of the disease’s progression – changes that are psychologically difficult and that present formidable barriers for individuals and health systems alike. While genetic predisposition may play a role in type II diabetes, its onset and severity can be modified by diet and activity. Complications can be reduced by addressing these risk factors and achieving blood pressure control and avoiding tobacco use.
To improve health in the next century, we will have to do a better job of applying the knowledge we already have and ensuring access to effective and economically affordable diabetes and HT care to the population that is essential for preventing, reducing diabetes and HT related complications. Certain measures are recommended to improve people’s perception and practice towards Diabetes and HT. A better-structured education programme is recommended to every individual especially those with diabetes and HT. The programme should cover topics such as symptoms, complications, preventive measures, diet and exercise. This should be done at all levels including through school, working centres and to the railway colony people.
A tailored programme with gradual introduction of exercise is encouraged with consideration of the individual’s age. A weight reduction programme incorporating diet modification is also recommended for those who are over weight, where as a weight maintenance programme is encouraged for those with normal body weight. A continuous self-monitoring system should be introduced for diabetic patients. This enables them to continuously monitor their blood glucose level as well as control their diet accordingly. studies on similar context but with wider scope and much larger sample size is recommended to confirm findings of this study and to further explore other relevant factors especially factors influencing practice and perception.
SUGGESTION AND RECOMMENDATION GOALS OF DIETARY THERAPY: 1) Restoration of optimal blood glucose and S.lipid levels. 2) Provision of adequate calories to maintain normal weight and Improvement of overall health in diabetes.
Three strategies in preventing coronary heart diseases in DM and HT Patients 1. Substituting unsaturated fats (poly unsaturated fats) for saturated fats and trans fats. 2. Increasing use of Omega-3 fatty acids from fish oil. 3. Diet rich in fruits, vegetables, nuts, and whole grains but low in refined grains.
CALORIES PRESCRIPTION: Calorie prescription is an important element in nutritional management. Calorie needs vary with age, sex and activity level. Recommended calorie level is based on individual’s desired weight. IDEAL BODY WEIGHT (IBW) KG =(HT IN CM - 100) X 0.9 CALORIE INTAKE BASED ON ACTIVITY IS AS FOLLOWS: SEDENTARY 20 - 25 CAL/KG (IBW) MODERATE 26 - 30 CAL/KG (IBW) STRENUOUR 31 - 35 CAL/KG (IBW)
An energy deficit of 500 k.cal/day will help to reduce 500 gms of weight every week. Dietary therapy for people with diabetes should be individualized with consideration given to usual eating habits and other lifestyle factors. Nutrition recommendations are implemented to attain the goals. Micronutrients such as vitamins and minerals are supplemented as required, sodium restriction in those with hypertension and cardiac failure. Diet with low glycaemic index is preferred to high glycaemic index. Complex carbohydrates are ideal as they are slowly digested and absorbed with lesser steep in raise of Post Prandial glucose and insulin response.
HEALTHY DIET/ BALANCED DIET Protein - 15 % of total energy Carbohydrates - 50 to 60 % of total energy Total fats - 25 to 35 % of total energy Saturated fat - < 7 % total energy Poly unsaturated fat - up to 10 % total energy Mono unsaturated fat - up to 20 % total energy Fiber diet - 20 to 30 grams per day Vitamins and minerals Water Salt - 2400 milligrams per day (One teaspoon of salt) Cholesterol - < 300 mgm/day
EXERCISE • Brisk walking, healthy diet will be helpful for longevity for people with Type2diabetes, and plays an important role in the prevention of over weight and obesity. TV watching is significantly associated with the risk of obesity and type 2 diabetes. Obesity can indirectly do some changes in the body which include the following: • Raising the levels of LDL (Bad cholesterol) • Lowering the levels of HDL (Good Cholesterol) • Raising the levels of Triglycerides • Increasing the Blood Pressure • Increasing the risk of Type 2 Diabetes
Exercise is known to • Increase insulin sensitivity, • Improve glucose tolerance, • Promote weight loss, • Reduce triglyceride levels • Increasing the levels of HDL cholesterol • Decreasing the levels of LDL cholesterol • Reduces the risk of hardening of arteries (atheroscelerosis) • Improving blood flow, which reduces the risk of infection in the lower legs and foot. People with diabetes are encouraged to exercise for at least 30 minutes, at least three or four times per week.
Exercise precautions: • Starting slowly and building up to longer/ harder workouts. • Keeping track of one’s heart rate. • Warming up slowly before exercise and cooling down slowly afterwards. • To calculate the maximum target heart rate (220 – One’s age), and maintain the 70% to 80% one’s maximum heart rate during exercise. • After exercise, the goal is to decrease the heart rate and relax the muscles by doing slow stretches. • To consult physician before beginning any exercise program. • To wear appropriate shoes and socks. • To have an exercise partner, snacks, and medical I.D card. • Testing glucose levels both before and after exercise.
YOGA FOR DIABETES • Types of yoga recommended for diabetes: • Pranayama • Dhanurasana • Ardha-Matsendrasana • Pachi motanasana • Halasana • And Vajarasana • Dhanurasana is most effective. These are practiced on an empty stomach for 30 minutes followed by shavasana for 10 –15 mts.
Effect of yoga Fall in FBS level Fall in PPBS level Reduction in systolic B.P Reduction in Diastolic B.P Reduction in dosage requirement of anti hypertensives Increase in HDL cholesterol Decrease in LDL cholesterol Decrease in free fatty acids Decrease in VLDL cholesterol Reduction in fasting insulin levels Increase in insulin receptors And Insulin sensitivity increases.