Download
1 / 19
240 likes | 623 Views
The Ubiquitous HLA System: applications in transfusion and transplantation. Dr Mary Purna Chacko Department of Transfusion Medicine and Immunohaematology Christian Medical College and Hospital, Vellore ISBTI 2012. Highly polymorphic cell surface molecules

E N D
The Ubiquitous HLA System: applications in transfusion and transplantation Dr Mary Purna Chacko Department of Transfusion Medicine and Immunohaematology Christian Medical College and Hospital, Vellore ISBTI 2012
Highly polymorphic cell surface molecules First identified and characterised in leukocytes The Human Leukocyte Antigen (HLA) System
HLA expression • Class I (HLA A, B and C)– all nucleated cells and platelets • Class II (HLA DR, DQ and DP)– B cells, activated T cells, macrophages, dendritic cells
Function of HLA molecules –Immune recognition peptide HLA Antigen presenting cell T cell
Allo-recognition DIRECT INDIRECT Recipient T cell Recipient T cell TCR TCR peptide Processing and presentation by recipient APC donor HLA peptide donor HLA Donor antigen presenting cell Recipient HLA Recipient antigen presenting cell
HLA typing • Serologyeg. HLA B7 • Molecular • low resolution – PCR SSP, PCR SSOP eg. HLA B*07 • Subtype– High resolution PCR SSP, PCR SSOP, SBT eg.HLA B*07:01 • Non coding polymorphisms - SBT eg.HLA B*07:01:01
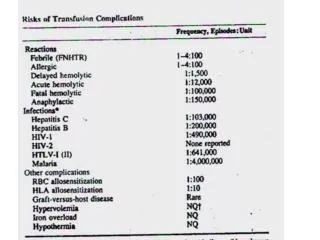
HUMORAL IMMUNITY Febrile non-haemolytic transfusion reaction (FNHTR) Immunological platelet refractoriness (IPR) Humoral graft rejection CELLULAR IMMUNITY Cellular graft rejection HLA related immune reactions OF RECIPIENT AGAINST DONOR TISSUE
HLA antibody mediated immune reactions Leukocyte Pyrogenic cytokines FNHTR Immunological platelet refractoriness Platelets Graft Hyperacute/acute graft rejection
HLA antibodies Induced by • Pregnancy • Transfusion • Transplantation
Prevention of allo-sensitisation Leuko-reduction • Prevents direct allo-recognition • Inhibits indirect allo-recognition • Removes antibody target in FNHTR UVB irradiation
The allosensitised patient -defining allosensitisation • Crossmatch • Mixed antigen screening assay • Percentage Panel Reactive Antibody (PRA)assay • Single antigen assay Does the patient have antibodies against this donor? Does the patient have anti-HLA antibodies? To what percentage of the population does the patient have antibodies? What is his chance of getting a compatible donor? What are the antigens against which the patient has antibodies? Which donors should be avoided?
Donor selection • Unmatched compatible donor • Crossmatch • Antigen negative approach – single antigen assay • HLA matchmaker 2.Matched donor
HLA inheritance Father Mother Haplotype A HaplotypeC Haplotype B Haplotype D Child 1 Child 2 Child 3 Child 4 Haplotype A Haplotype A Haplotype B Haplotype B HaplotypeC Haplotype D HaplotypeC Haplotype D Chance of having an HLA identical sibling =1-(0.75)n
HLA related immune reactions OF DONOR AGAINST RECIPIENT • Transfusion associated acute lung injury (TRALI) • Transfusion associated graft versus host disease (TA GVHD)
TRALI Anti HLA/HNA antibody Chemotactic factors neutrophile Endothelial cell Pulmonary edema Adherence to pulmonary endothelium/epithelium
Antibodies most commonly found in multiparous women Avoid use of female donor plasma* *Eder et al (Transfusion 2010); Nakazawa et al (Transfusion 2009) PREVENTION OF TRALI
Graft versus Host Disease • Transfer of viable lymphocytes • Inability of host to mount immune response • Sharing of HLA haplotypes prevents recipient from recognising donor tissue as foreign A2 B7 A2 B7 A2 B7 A3 B35
Prevention of graft versus host disease • Choosing HLA matched donors • Irradiation – Inactivates viable lymphocytes
If we cannot end our differences, at least we can make the world safe for diversityJohn F. Kennedy