Download
1 / 55
550 likes | 744 Views
St. Gallen March 11-14, 2009. Roma 11 Giugno 2009 Teresa Gamucci Oncologia Medica Sora (FR). St. Gallen: Overview. 11 th international conference “Primary Therapy of Early Breast Cancer: Evidence, Controversies, Consensus” 4500 participants Expert panel includes 40 Top KOLs

E N D
St. Gallen March 11-14, 2009 Roma 11 Giugno 2009 Teresa Gamucci Oncologia Medica Sora (FR)
St. Gallen: Overview • 11th international conference “Primary Therapy of Early Breast Cancer: Evidence, Controversies, Consensus” • 4500 participants • Expert panel includes 40 Top KOLs • 22 EU, 13 US, 4 from other countries • Outcome to be published as expert consensus recommendations in Annals of Oncology later this year
Use of Chemotherapy in Hormone Receptor-Positive Disease • Increasing attention to this topic • Need to identify patients who can be spared unnecessary chemotherapy toxicity • Decision based according to • Risk assessment (e.g. nodal status, grade) • Tumor biology • Genomic profiling
Paradigm of Endocrine Responsiveness Endocrine Responsiveness Uncertain Sure Absent • ER and PR low/intermediate and/or any of these: • PgR absent • UPA / PAI-1 high • HER2 overexpressed • Increased proliferation • High grade Both receptors high levels No No No No No ER and PR absent May not differ if N0 vs N+ Chemo only option Chemo adds to hormonal Consider chemo
Can We Identify HR+ Patients Who Do Not Need Chemotherapy • Old methods are still beneficial but insufficient • Grade • Nodal status • ER / PgR status • Increasing interest/evidence for molecular risk assessment • Biological markers ( Ki 67, mitotic index etc.) • New methodologies, e.g. multigene assays etc.
Use of Multigene Assays Panel Vote 2009 The panel accepts the use of molecularly-based tools, if readily available, as an adjunct to high-quality standard histo-pathologic assessment in patients with ER+ breast cancer when the doctor and patient are uncertain or ambivalent about the administration of adjuvant chemotherapy Optimally, the patient should be enrolled in appropriate trials 80% YES18% NO
Anthracycline vs Non-Anthracycline Regimens • Are anthracyclines a necessary component for effective chemo regimens? • NO 61% (but useful in some situations) • USON 06090 (TC vs. TAC) trial will answer the question (for HER2- population)
Anthracycline vs Non-Anthracycline Regimens Are non-anthracycline regimens accepted as a standard treatment? • In HER2+ population: • 2007: Slim majority found TCH to be an acceptable alternative • 2009: Though BCIRG 006 not yet published, data accepted as solid proof • Is there a different standard chemo regimen for HER2+ disease? YES 33% NO 51% • In HER2- population: • Is TC x 4 a standard adjuvant regimen? YES 43%
Stima dell’effetto epidemiologico di trastuzumab a 10 anni in 5 paesi europei
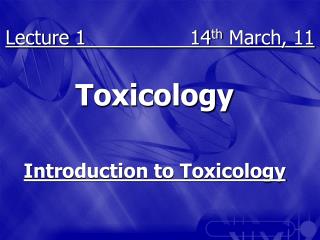
St Gallen guidelines: HER2 positivity alone confers either intermediate- or high-risk status HER2 is recognisedin guidelines as an independent risk factor Even in T1N0 disease, HER2-positive status is associated with a significant risk of relapse Breast cancer-specific survivalin T1pN0 cohort (Norris, et al) 1.0 0.8 0.6 0.4 0.2 0 HER2 negative HER2 positive Breast cancer-specific survival Patients untreated with trastuzumab p=0.031 0 2 4 6 8 10 12 Time (years) Joensuu, et al. Clin Cancer Res 2003; Norris, et al. SABCS 2006 Goldhirsch, et al. Ann Oncol 2007
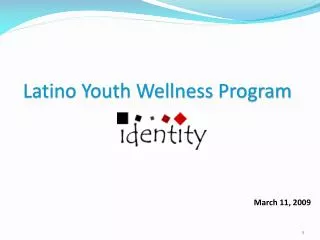
Più di 13.000 pazienti arruolate in 4 studi clinici multicentrici in adiuvante Docetaxel + carboplatin Docetaxel Trastuzumab Paclitaxel Standard CTx HERA (ex-USA) BCIRG 006 (global) Observation IHC / FISH (n=5,090) FISH(n=3,222) 1 year 1 year 2 years 1 year NCCTG N9831 (USA) NSABP B-31 (USA) IHC / FISH (n=2,030) IHC / FISH (n=3,505) 1 year 1 year 1 year Doxorubicin + cyclophosphamide IHC, immunohistochemistry FISH, fluorescence in situ hybridisation CTx, chemotherapy Piccart-Gebhart et al 2005 Romond et al 2005; Slamon et al 2006
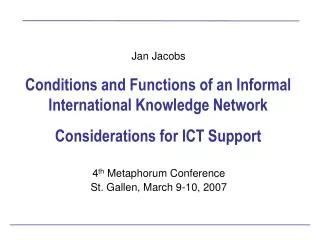
HERA: trastuzumab significantly improves DFS 6.3% 100 80 60 40 20 0 1 year trastuzumab Observation Patients(%) 3-yearDFS Events HR 95% CI p value 80.6 218 0.54–0.76 <0.0001 0.64 74.3 321 0 6 12 18 24 30 36 Months from randomisation No. at risk 1,703 1,591 1,434 1,127 742 383 140 1,698 1,535 1,330 984 639 334 127 Smith, et al. Lancet 2007 DFS = disease-free survival
Trastuzumab ha determinato una riduzione di un terzo del rischio di morte Overall survival benefit Median follow-up, years HERA CTxH 1 year 2 3 B-31 / N9831 ACPH 3 BCIRG 006 ACDH BCIRG 006 DCarboH 3 FavoursTrastuzumab Favours noTrastuzumab 0 1 2 HR Size of square represents sample size; horizontal bars indicate 95% confidence intervals H, Trastuzumab; AC, doxorubicin, cyclophosphamide P, paclitaxel; D, docetaxel; Carbo, carboplatin HR, hazard ratio Slamon et al 2006 Perez et al 2007; Smith et al 2007
Trastuzumab migliora DFS indipendentemente dalla dimensione del tumore HERA 0-2 cm >2-5 cm >5 cm N9831 / B-31 0-2 cm >2-5 cm >5 cm BCIRG 006 ACDH <2 cm ≥2 cm DCarboH <2 cm ≥2 cm 0.0 0.5 1.0 1.5 2.0 2.5 Favours Trastuzumab Favours no Trastuzumab HR Slamon et al 2006 Perez et al 2007; Smith et al 2007 DFS, disease-free survival
Trastuzumab migliora la DFS indipendentemente dallo stato linfonodale N- HERA 1-3+ nodes ≥4+ nodes Not assessed N9831 / B-31 N- 1-3+ nodes 4-9+ nodes >10+ nodes BCIRG 006 N- ACDH N+ N- DCarboH N+ 0.0 0.5 1.0 1.5 2.0 2.5 Favours Trastuzumab Favours no Trastuzumab HR Slamon et al 2006 Perez et al 2007; Smith et al 2007 N, node
Trastuzumab migliora la DFS indipendentemente dall’età del paziente HERA <35 years 35-49 years 50-59 years ≥60 years <40 years N9831 / B-31 40-49 years 50-59 years ≥60 years 0.0 0.5 1.0 1.5 2.0 2.5 Favours Trastuzumab Favours no Trastuzumab HR Perez et al 2007; Smith et al 2007
Qual è la durata ottimale del trattamento con Trastuzumab? 0.10 0.02 0.12 0.14 0.16 0.18 0.08 0.06 0.04 100 0 40 20 0.008 0.006 0.004 0.010 0.012 80 60 120 Observation 1 year H 24 30 0 12 18 6 36 0 48 42 4 3 2 1 HERA PACS-04 HR HR HR=0.5795% CI (0.30-1.09) HR=1.04 Observation 0.002 1 year H 0.00 1-6 7-12 13-18 19-24 25-30 31-36 Months Months since randomisation NSABP B-31 / NCCTG N9831 Rate per1,000 women/year AC→T AC→TH Romond et al 2005Smith 2006Spielmann et al 2007 Years since randomisation
Pazienti HER2+ con tumore < 1 cm Quesiti aperti
Trastuzumab è indicato dalla linee guida come cardine per il trattamento delle pazienti HER2+ Trastuzumab permette elevate percentuali di guarigione nei pazienti con carcinoma mammario HER-positivo operabile Il vantaggio della terapia con Trastuzumab è stato osservato in tutti i pazienti, indipendentemente dalle variabili prese in considerazione (età, stadio, tipo di chemioterapia) Il netto beneficio del trattamento con Trastuzumab compensa di gran lunga il rischio di eventi cardiaci, nella maggior parte dei casi reversibili e facilmente trattabili Attualmente 52 settimane di trattamento con Trastuzumab rappresentano la durata standard della terapia Key-messages
L’analisi più dettagliata dello studio HERA sulla popolazione anziana evidenzia che l’efficacia di Trastuzumab è simile rispetto alla popolazione generale (DFS 85.7% vs 87%) Key-messages (2)
USON 9735: 7-Year Update OS DFS Jones et al. J Clin Oncol. 2009
Medico-Marketing Comments • Non-anthracycline regimens are gaining ground both in Her2 positive and Her2 normal segments • Even if TCx4 is not recognized as the standard, it is highly (43%) accepted as a viable option • For which patients are doctors ready to spare anthracyclines in everyday clinical practice? • The question remains open
What’s New • FinHER update • HERA landmark analysis • Consensus panel discussion
FinHER 5-year Update FinHer: Study Design If HER2+ Docetaxel 100 mg/m2 q3w x 3 → FE60C q3w x 3 Trastuzumab q wk x 9 R R No trastuzumab Vinorelbine 25 mg/m2 D1, 8, 15 q3w x 3 → FE60C q3w x 3 N=1010 Trastuzumab administered concomitant with docetaxel or vinorelbine treatment • Patient population: • Node-positive or • Node-negative with T > 2 cm and PgR- • Age ≤ 65 years • Stratification factors: • HER2 status • Institution 62 months final analysis
FinHER 5-year Update Distant Disease-Free Survival (5-y)
FinHER 5-year Update Overall Survival (5-y)
FinHer Authors’ Conclusions • Adjuvant treatment with docetaxel improves DDFS compared to vinorelbine. • A brief course of trastuzumab administered concomitantly with docetaxel is safe and effective, and warrants further evaluation.
HERA Study Design HERA Update Herceptin q3w x 2 years HER2-positive early breast cancer(IHC 3+ and / or FISH+)n=5102 Surgery + (neo)adjuvant chemotherapy + radiotherapy Herceptin q3w x 1 year Observation Option to cross over to Herceptin (after IA 2005)
HERA Update DFS (ITT): 4-year Median Follow-up Patients (%) 100 1-year Herceptin 80 6.4% Observation 60 40 4-yearDFS 72.278.6 Events 458369 HR 0.76 95% CI 0.66, 0.87 p value <0.0001 20 0 0 6 12 18 24 30 36 42 48 Months from randomisation No. at risk 16981703 15641619 14401552 13631485 12971414 12401352 11801280 9921020 712854
OS (ITT): 4-year Median Follow-up HERA Update 1-year Herceptin Patients (%) 100 1.6% Observation 80 60 40 4-yearDFS 87.789.3 Events 213182 HR 0.85 95% CI 0.70, 1.04 p value 0.1087 20 0 0 6 12 18 24 30 36 42 48 Months from randomisation No. at risk 16981703 16421660 16011640 15561615 15191577 14711524 13981447 11751149 828953
DFS and OS Over Time HERA Update Median follow-up (% follow-up time after selective crossover) Median follow-up (% follow-up time after selective crossover) No. of DFS eventsH 1 year vs observation No. of deathsH 1 year vs observation DFS benefit OS benefit 200511 year(0%) 200511 year (0%) 127 vs 220p<0.0001 29 vs 37p=0.26 200622 years(4.1%) 200622 years (4.3%) 59 vs 90p=0.0115 218 vs 321p<0.0001 20084 years (33.8%) 20084 years(30.9%) 182 vs 213p=0.1087 369 vs 458p<0.0001 0 1 2 0 1 2 FavoursHerceptin Favours noHerceptin FavoursHerceptin Favours noHerceptin HR HR 1Piccart-Gebhart et al 2005; 2Smith et al 2007
Landmark Analysis HERA Update • Thelandmarkanalysisconsidersonlypatientswhowerealiveanddiseasefreeon16May2005 • N=885patientsinobservationgroupwhoswitchedtoHerceptin(randomizedto1or2years) • N=469patientsinobservationgroupwhodidnotcrossover • 90%ofpatientswhoswitchedtoHerceptindidsoat~9months • Specificquestionsaddressed: • WhatwasthecourseofdiseaseinthesubgroupsofobservationpatientswhodidordidnotcrossovertoHerceptin? • IsthereanyeffectofthelateintroductionofHerceptin?
HERA Update Observation: Alive and disease free on 16 May 2005 Selective crossover No crossover Months from randomisation 1354 1353 1339 1316 1278 1239 1180 992 712 DFS: Observation (alive, no DFS event)Selective Crossover and No Crossover Patients alive and disease free (%) 100 80 60 40 20 0 0 6 12 18 24 30 36 42 48 No. at risk 885 885 884 878 870 851 822 690 480 469 468 455 438 408 388 358 302 232
HERA Update OS: Crossover vs No-crossover Patients alive (%) 100 80 60 40 Observation: Alive and disease free on 16 May 2005 20 Selective crossover No crossover 0 0 6 12 18 24 30 36 42 48 Months from randomisation No. at risk 1354 1354 1350 1344 1332 1316 1270 1065 759 885 885 885 883 881 875 852 718 499 469 469 465 461 451 441 418 347 260
HERA 4-year Follow-up Data: Summary (1) HERA Update • The updated analysis at 4 years was limited to 1-year Herceptin vs observation as recommended by IDMC • Extensive selective crossover of observation patients to active therapy biased the ITT comparison • Landmark analysis of observation patients who were disease free on 16 May 2005 explored the effects of later introduction of Herceptin • Lack of randomisation limits the interpretation of the landmark analysis • different outcome due to drug effect or patient characteristics?
HERA 4-year Follow-up Data: Summary (2) The DFS benefit associated with Herceptin is maintained at 4-year median follow-up 50% of patients in the observation arm crossed over to Herceptin treatment, therefore the OS benefit is no longer statistically significant Patients crossing over at a later date appear to benefit from 1 year of Herceptin HERA Update
Cardiac Safety Update in Adjuvant Trastuzumab Trials a Patients who crossed over are censored from the data of starting trastuzumab treatment
HERA Trial: Cardiac Safety in Observation Group a For 3 of the patients, the LVEF drop occurred after 16 May 05 and may have influenced the patient decision
Concomitant vs. Sequential Panel Vote 2009 • No formal voting • Panel considered both approaches as reasonable • Increasing body of clinical evidence for concomitant use
NCCTG N9831 (Coming ASCO 2009) AC q3w x 4 Paclitaxel qw x 12 RANDOMIZATION N=3595 AC q3w x 4 Paclitaxel qw x 12 • Patient Population • N+ or high-risk N- breast cancer • HER2+ (IHC 3+ or FISH) Trastuzumab qw x 52 AC q3w x 4 Paclitaxel qw x 12 Trastuzumab qw x 52
Optimum Trastuzumab Duration • St. Gallen 2007: standard duration trastuzumab accepted as 1 year • No panel vote 2009 • Ongoing clinical trials to define optimal duration • SOLD: 9 weeks vs. 1 year, n=3000 • ShortHER: 9 weeks vs. 1 year, n=2500 • PHARE: 6 mo vs. 1 year, n=3500 (2400 enrolled to date); any adjuvant chemotherapy
Key Messages • Trastuzumab is effective up front or after chemo • Cardiac toxicity: • Minimal with short duration (FINHER) treatment • Remains even when trastuzumab is administered long after the end of chemotherapy (HERA landmark analysis) • Concomitant use is gaining ground due to clinical evidence • BCIRG 006 to be published • NCCTG to be presented at ASCO 2009? (LBA) • Duration of trastuzumab treatment • 1 year still recommended as standard • Trials ongoing to evaluate short- vs long-term duration