Download
1 / 28
280 likes | 475 Views
MDHA Professionals’ Forum: Acquired Brain Injury and Substance Use. Robert Campbell AOD/ABI Clinical Consultant Southern Metropolitan Region. What is Acquired Brain Injury (ABI) ?. The term ABI is used to describe all types of brain injury that occur after birth.

E N D
MDHA Professionals’ Forum:Acquired Brain Injury and Substance Use Robert Campbell AOD/ABI Clinical Consultant Southern Metropolitan Region
What is Acquired Brain Injury (ABI) ? • The term ABI is used to describe all types of brain injury that occur after birth. Other terms you may hear include: • TBI: Traumatic Brain Injury • ABI: Acquired Brain Impairment • HI: Head Injury • ARBI: Alcohol Related Brain Injury • SRBI: Substance Related Brain Injury
Common Causes of ABI • Accidents –road, sporting or work related • Assaults • Falls, often secondary to intoxication • Strokes, can be secondary to substance use • Substance use – 10 years of daily use is a general rule of thumb • Lack of oxygen (hypoxia) – interruption of oxygen supply to the brain during heart attack, seizures, such as from epilepsy, drug overdose, suffocation or near drowning, attempted hanging or suicide attempt. Loss of consciousness greater than 30 minutes. • Brain Tumours • Infections such as meningitis (infection of the brain covering) and encephalitis (infection of the brain tissue itself).
Alcohol is involved in more than 50% head injuries Of those patients with head injuries, 25-65% have a history of substance abuse Up to 50% of patients return to pre-injury consumption levels 14% develop substance abuse problems after head injury 80% of clients in AOD treatment will show signs of cognitive impairment The prevalence of alcohol related brain injury in the Australian population is 2% Australia has higher rates of alcohol related brain injury than any other western country Prevalence of AOD/ABI
Spectrum of AOD/ABI Mild - 85% Moderate - 10% Severe - 5%.
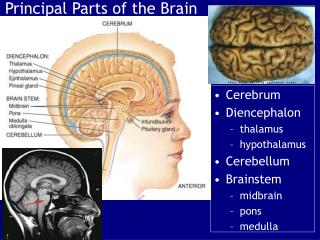
Common AOD Related ABI Impairments Executive / Frontal Lobe Functions • Capacity to learn from mistakes • Problem solving • Planning and organising • Seeing consequences in behaviour • Putting plans into action • Impulsiveness & disinhibition • Making new decisions • Intoxication/Chaotic Substance Use Life Style or ABI?
Complex & Interacting Issues Delusions & Hallucinations Medication Suicidality Anxiety Trauma Side-Effects Hospitalisation Stress Depression Age Culture HIV / Hepatitis Family Licit & Illicit AOD use Gender Legal charges Availability of AOD Peers Tolerance Homelessness Pattern of Use Unemployment Treatment Experiences Prison Income
No wonder, then, that ABI/AOD can seem like a bit of a… But this need not be the case…
ABI/AOD Clinical Consultants Leah Mammino AOD/ABI Clinical Consultant Eastern Metropolitan Region
Relevant Issues from Strategic Plan 2001 DHS Studies across regions in Victoria prior to 2001 found: • Lack of specific ABI knowledge & awareness of ABI in the service system. • Lack of training for existing workers and carers/family. • Lack of formal links between agencies assisting people with an ABI. • Lack of clearly identifiable centre of expertise within each region. (ABI Strategic Plan, DHS, 2001 )(Source: Deane, 1998; Honey & McCubbery, 1997; Collins, 1996; Dickman & MacPhail, 2000).
Challenges of working with AOD/ABI Clients Heterogeneous group Complex presentations with limited service responses – “silo effect” Tendency to “fall through the gaps” Resource intensive Challenging to services and clinicians, with such clients often being misinterpreted and misunderstood.
Development of Nine ABI/AOD Clinical Consultant Positions • Four positions allocated to each Metropolitan Region in Melbourne (North, South, East and West) • 5 positions allocated across regional Victoria (Gippsland, Hume, Barwon ‘Geelong’, Loddon Mallee ‘Bendigo’, Grampians)
Regions in Victoria Mildura NORTH WESTERN Shepparton Bendigo WESTERN CENTRAL NORTH EASTERN Horsham Ballarat SOUTH EASTERN METRO SOUTH WESTERN Melbourne Morwell Geelong Warrnambool
Objectives of ABI/AOD Clinical Consultants • Identify clients with ABI already in the drug treatment system • Facilitate access for clients with ABI in need of treatment • Keep clients with ABI in the service system by introducing appropriate models of treatment to AOD clinicians • Gauge numbers of clients with ABI’s receiving treatment in the AOD sector – (60% -80%) • Determine resources needed to facilitate treatment of this client group • Build capacity through provision of ABI training
Role of the ABI Clinical Consultant • To facilitate links between the ABI & AOD service sectors • To provide secondary consultation to ABI & AOD clinicians • To advocate on behalf of clients, families & ABI services for access to & treatment in AOD services and vice versa • Have a small caseload of ABI clients with AOD issues • Provide ABI training
So, what are some ways of Identifying AOD/ABI? • Consistently screen for ABI • Encourages good, targeted history taking identifying risk factors for ABI • Can be used as a decision making tool for whether a neuropsychological assessment is warranted • An ABI screening tool is not diagnostic.
Clinical Treatment Guidelines http://docs.health.vic.gov.au/docs/doc/Clinical-treatment-guidelines-for-Alcohol-and-Drug-Clinicians---Co-occurring-acquired-brain-injury---cognitive-impairment-and-alcohol-and-other-drug-use-disorders---2006 Page 75 has the AOD/ABI Screening Tool
Managing Cognitive Impairments in Counselling AOD Counselling can be effective with mild to moderate ABI: • The counsellor more directive, but joining with client; • Emphasis on behavioural strategies – Concrete approach, less emphasis on emotional processing and abstract approaches; • Counselling not as effective for severe cognitive impairment due to diminished insight and awareness; • Professional self-care - supervision, reflective practice. • Seek assistance from ABI Behaviour Consulting!
Getting Information • Neuropsychological assessments (where appropriate) • OT Assessments • Collateral information from family & significant others • Other treatment, agencies & services
Successful Referral, Shared Care and Consultation • Follow-up referrals • Work collaboratively with services in a shared care framework ( i.e IRP’s) • Draw on secondary consultation from relevant services if needed.
What are some ABI Services? Specialist neuropsychological assessment eg ARBIAS Case management services eg ARBIAS, Melbourne City Mission, LIAISE Specialist ABI Consultancy services eg ABI Behaviour Consultancy, AOD/ABI Clinical Consultants, CBDATS Specialist Counselling services egBouverie Centre ABI Family counselling DHS Disability Client Services DHS Regional Complex Care.
Thank You. Leah Mammino AOD/ABI Clinical Consultant Eastern Metropolitan Region Eastern Drug and Alcohol services lmammino@monashlink.org.au 1300 552 509