Download
1 / 25
250 likes | 371 Views
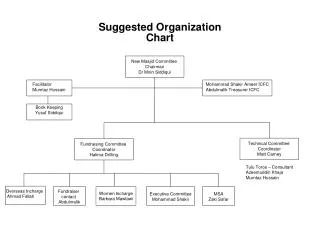
OPSE-suggested answer. Prepared by: Dr. HK Ngan PMH AED. Case 1. M/65 PH:DM, HT Attended AED because of abdominal distension and constipation for two days. Case 1. Case 1. 1) Describe the x-ray findings? 2) What is the diagnosis? 3) What are the main complications of this condition?

E N D
OPSE-suggested answer Prepared by: Dr. HK Ngan PMH AED
Case 1 • M/65 • PH:DM, HT • Attended AED because of abdominal distension and constipation for two days
Case 1 • 1) Describe the x-ray findings? • 2) What is the diagnosis? • 3) What are the main complications of this condition? • 4) Name three predisposing factors for this condition? • 5) What is the treatment?
Case 1-suggested answer • 1) a loop of dilated(1) large(1) bowel pointing toward the diaphragm with demonstration of “coffee bean” (2)sign or “bent inner tube”(2) sign (4 mark) • 2) Sigmoid volvulus (2) (2 mark) • 3) bowel obstruction(1),perforation(1),bowel ischaemia(1) • (3 mark) • 4) Redundant sigmoid colon with narrow mesentery, chronic constipation, Chacas disease(trypanosomiasis), Parkisonism, spinal cord disease, mental illness, high fiber diet, high altitude (3 mark) • 5) Sigmoidoscopy(1) and insertion of rectal tube(1) for decompression; operative (1)management and resection • (3 mark)
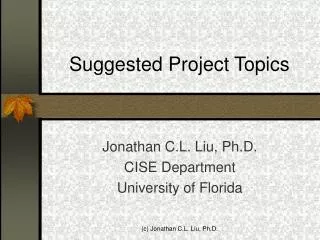
Case 2 • Nigerian tourist • F/42 • Brought in by police from airport for abdominal pain
Case 2 • 1) Describe the x-ray findings? • 2) What is the diagnosis? • 3) What will be the complication of this condition? • 4) What is your management?
Case 2-suggested answer • 1) Bowel is not dilated; no air-fluid level; multiple oval soft tissue(packet)homogenous shadows (2)inside the bowel with rim of halo(1) “double condom sign”(2) (4 mark) • 2) Body packing, body stuffing, internal carrier, balloon swallower (any one) (2 mark)) • 3) bowel obstruction(1); toxicity (1)due to rupture of contained drug (2 mark) • 4) Asymptomatic: Whole bowel irrigation(1) and laxative(1) (2 mark) Symptomatic: i)Operative intervention(1) in case of obstruction(1), retention(1) of packet and sign of leakage/rupture(1) of packet ii) Antidote administration(1) (5 mark)
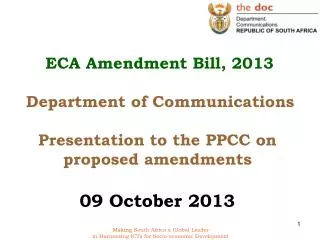
Case 3 • PH: Good • M/50 • Presented to AED for chest pain on and off for 3 weeks. Now symptoms free. • Serial Troponin I<0.03 (not rasied)
Case 3 • 1) What is the ECG findings ? • 2) What is the diagnosis? • 3) What is the significance of this condition and what will be the complication? • 4) What is the best treatment for this condition and why?
Case 3-suggested answer • 1) NSR; HR 60/min;PR interval normal; QRS not widen ; Axis normal ; TWI at V3,V4 (either one 1 mark); biphasic T wave inversion at V3 V4(2) (3 mark) • 2) Wellens syndrome (2 mark) • 3)Critical proximalLAD stenosis and preinfarction stage of coronary artery disease; left untreated may proceed to anterior wall infarction of resulting in serious ventricular dysfunction, CHF and death (7 mark) • 4) Urgent coronary angiography and revascularization(2) as 75 % of this patient will proceed to AMI(1) even with medical treatment (aspirin, beta-blocker therapy, nitroglycerin, morphine, heparin, clopidogrel, and glycoprotein (GP) IIb/IIa inhibitors) (1) (3 mark)
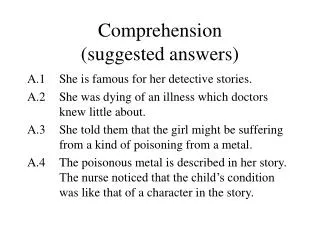
Case 4 • F/40 • Brought in by mother with abnormal behavior and delusional idea for one month. No history of head injury.
Case 4 A C D B
Case 4 • 1) What is the CT findings? • 2)Give 3 differential diagnosis from the CT finding? • 3)Give the cistern/fissure name of A,B, C, D • 4)What physical examination you would emphasis with this CT findings? • 5)What other investigation you would like to do to confirm your suspicion?
Case4- suggested answer • 1) A mass leision over the suprasellar region (2); ( 2mark) • 2) Pituitary adenoma(macroadenoma); aneurysm; craniopharyngioma; meningioma; Rathke’s cyst ;chiasmatic glioma ; dermoid; epidermoid,schewannoma;geminoma; metastasis (any three) (3 mark) • 3)A-Suprasellar cistern ; • B-Circummesencephalic (ambient) cistern • C-Sylvian cistern/fissure • D- Quadrigeminal cistern (4 mark) • 4)Visual field & acuity exam; fundi; neurological exam (3 mark) • 5) CT brain with contrast; MRI; Angiogram (3 mark)
Case 5 • 63/M • Construction site worker • Right eye being splashed by liquid concrete (cement) • Used tap water to rinse it briefly • C/O pain, tearing, blurring of vision
Case 5 • Describe the clinical findings from the photo. • What is the likely culprit chemical causing such injury? • Name one essential bedside test. • Which will have more serious injury, acid or alkali? Give your explanation • How would you grade the severity of this injury?
Case 5 –suggested answers • Injected conjunctiva/ hazy cornea/ FS +ve with epithelial defect at cornea (3 mark) • Lime or calcium hydroxide ( CaOH2) causing alkali burn (3 mark) • pH in the conjunctival sac (1 mark) • Alkali.(1) Alkali will have more damage because alkaline penetrates faster and deeper than acid through the cornea. The fatty acids in cell membranes are broken down into soap and glycerol by the process of saponification.Whileacids result in coagulative necrosis at surface and form a protective barrier to prevent further penetration ( 4 mark) 5. Determined by severity of cornea injury, extensiveness of limbal involvement and percentage of conjunctival involvement The Roper-Hall(1) classification on the degree of corneal involvement(1`) and limbal ischemia(1). The Dua(1) classification on an estimate of limbal involvement (in clock hours)(1) and the percentage of conjunctival involvement(1). (4 mark)