Download
1 / 8
90 likes | 384 Views
Osteonecrosis of the Femoral Head. Matthew Orton Radiology Presentation 7/20/2007. HPI. A 20 yo male with SLE reports to ER complaining of chronic L hip pain and new L knee pain that has not resolved since fall 1 week ago. PCP diagnosed SLE in 2004.

E N D
Osteonecrosis of the Femoral Head Matthew Orton Radiology Presentation 7/20/2007
HPI • A 20 yo male with SLE reports to ER complaining of chronic L hip pain and new L knee pain that has not resolved since fall 1 week ago. • PCP diagnosed SLE in 2004. • Meds: Lisinoprol, Prednisone, Zantac, HCTZ, Imuran, Volteran,
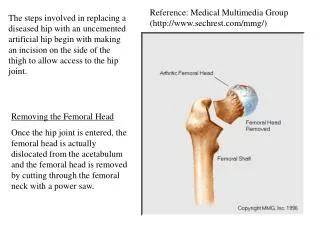
Sclerosis and density changes • “Crecent Sign” = subcondral radiolucancy • Loss of smooth spherical or collapse of femoral head. • Joint space narrowing , degenerative changes.
MRI of Femoral Head Osteonecrosis • Coronal T1 MRI of both hips shows diffuse low signal throughout the left femoral head, neck, and proximal shaft. • Axial T2 MRI of both hips shows diffuse high signal in the left femoral head consistent with the avascular necrosis. Images from: brighamrad.harvard.edu
Osteonecrosis of Femoral Head • Osteonecrosis = aseptic necrosis, avascular necrosis, ischemic necrosis and osteochondritis dessicans. • Mechanism compromise of bone vasculature leading to death of bone and marrow cells and ultimately mechanical failure. Process is often progressive and results in joint destruction in 3-5 years if untreated. • Exact pathogenesis still under debated. Some theories include intravascular necrosis, increased intraosseous pressure, mechanical stresses, or metabolic factors. • Prevalence is 10,000-20,000 cases diagnosed in US/year. M:F = 8:1. 5% of patients with SLE will develop osteonecrosis. • Staging • Stage 0 — All diagnostic studies normal, diagnosis by histology • Stage 1 — Plain radiographs and computed tomography normal, magnetic resonance imaging positive and biopsy positive. • Stage 2 — Radiographs positive but no collapse. • Stage 3 — Early flattening of dome, crescent sign, computed tomography or tomograms may be needed. • Stage 4 — Flattening of femoral head with joint space narrowing, possible other signs of early osteoarthritis
Treatment of Osteonecrosis of Femoral Head • Conservative management ( rest and pain control) if <15% femoral head involved. • Bisphosphonates can slow progression • Core decompression may slow progression. • Osteotomy move areas of necrosis away from major load bearing and try to redistribute on healthy bone. • Joint replacements (higher rate of complications and revisions)
References • Donohue, JP.UptoDate: Osteonecrosis (avascular necorsis of bone). 2007. • Jones LC, Hungerford DS. Osteonecrosis: etiology, diagnosis, and treatment. Curr Opin Rheum 2004; 16: 443-449. • Galindo M, Mateo I, Pablos JI. Multiple avasular necrossis of bone and polyarticular septic arthritis in patients with systemic lupus erythematosus. Rheumatol Int 2005; 25: 72-76.