Download
1 / 46
480 likes | 1.15k Views
References. ??????? ?? ??????????Clinical practice guideline : management of sinusitis : AMERICAN ACADEMY OF PEDIATRICS :Volume 108, Number 3 :September 2001SINUSITIS IN CHILDREN : Dept. of Otolaryngology, UTMB, Grand Rounds ,Kyle L. Kennedy, M.D. November 1, 1995 Up to date 13.1. Sinuses

E N D
1. Sinusitis in children Presented by
Theera Rojanapremsuk
2. References ??????? ?? ??????????
Clinical practice guideline : management of sinusitis : AMERICAN ACADEMY OF PEDIATRICS :Volume 108, Number 3 :September 2001
SINUSITIS IN CHILDREN : Dept. of Otolaryngology, UTMB, Grand Rounds ,Kyle L. Kennedy, M.D. November 1, 1995
Up to date 13.1
3. Sinuses Sinuses are moist air spaces within the bones of the face around the nose
Human have 4 pairs of sinuses
The ethmoid and the maxillary sinuses form in the third to fourth gestational month
The sphenoid sinuses are generally pneumatized by 5 years of age
the frontal sinuses appear at age 7 to 8 years but are not completely developed until late adolescence.
5. Sinusitis
6. Sinusitis Sinusitis is the inflammation/infection of 1 or more paranasal sinuses
It is traditionally subdivided into
- acute (symptoms lasting <3 wk)
- subacute (symptoms lasting 3 wk to 3 mo)
- chronic (symptoms lasting >3 mo).
7. Anatomy and physiology The maxillary, ethmoid, frontal and sphenoid are air-containing spaces that are lined by pseudostratified, columna epithelium bearing cilia
The sinus mucosa contain goblet cells, which secrete that aids in trapping inhales particle and debris
10. Osteomeatal complex
11. Pattern of the mucociliary clearance is essential for the proper health of the function of the paranasal sinuses (PNS)
The middle meatus is functional importance , as it serves as a drainage pathway for the maxillary, ethmoid and frontal sinuses
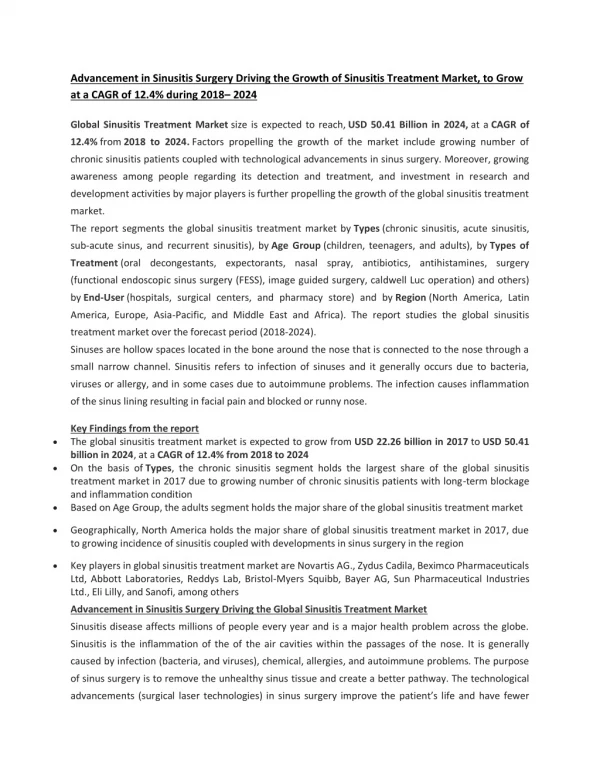
12. Epidemiology An estimated more than 30 million patients in US have sinus disease.
Although the exact incidence of sinusitis in the pediatric population is unclear
Upper respiratory infections (URIs) are one of the most common presentations
A viral infection associated with the common cold is the most frequent etiology of acute sinusitis
Approximately 5-13% of URTIs are complicated by bacterial sinusitis
13. Pathogenesis
15. Predisposing factors 1. Local factor
- cold or rhinitis - allergy
- nasal polyp - foreign body
- deviated of nasal septum
2. Systemic factor
- cystic fibrosis
- defective ciliary function
- immuno- compromised host
16. Microbial etiology Viruses are the most frequent cause of rhinosinusitis
viruses are known to predispose to subsequent bacterial infection via such mechanisms as viral-induced impairment of the mucociliary apparatus.
17. Microbial etiology
18. Diagnosis Sign and symptom
Physical examination
Radiologic tests
19. sign and symptom of sinusitis Nasal congestion
Purulent discharge
Maxillary tooth discomfort
Hyposmia
Facial pain or pressure that is worse when bending forward
21. Sign and symptoms In pediatric patients, most URIs last 5-7 days.
By 10 days, the URI almost always improves.
Most rhinoviral infections improve within 7-10 days so the complaint of persistent or worsening symptoms may indicate a developing bacterial sinusitis.
Pediatric patients may complain of a daytime cough and persistent nasal discharge.
Complaints of facial pain and headache are rare in children.
22. Younger kids typically have cold-like symptoms, including a stuffy or runny nose and slight fever
if child develops a fever after the third or fourth day after cold symptom begin, it could sinusitis
In older children and teens, the most frequent symptoms of sinusitis are a daytime dry cough that doesn't improve after the first 7 days of cold symptoms, fever, worsening congestion, dental pain, ear pain, or tenderness in the face.
24. Physical examination - Facial tenderness to palpation is present
- Nasal mucosa is inflammation, redness and swelling
- Purulent secretions in the middle meatus (highly predictive of maxillary sinusitis)
- Complete opacification of sinus on transillumination is present.
27. Radiologic tests Plain film
CT scan
MRI
28. Plain film - caldwell for frontal and ethmoid
- Water�s for maxillary and sphenoid
- submentovertex and lateral for
sphenoid
31. Plain film
33. CT scan - CT scanning is the criterion standard for evaluation
- Indications for obtaining a CT of the sinuses include
1. evidence of severe, persistent sinus disease following maximal medical therapy
2. sinus disease in the immunocompromised patient
3. suspicion of a suppurative complication of sinus disease.
34. CT scan
36. Therapy Non-medical treatment
Medical theray
Surgical therapy
37. Supportive treatment Avoid cigarette smoking
Drink plenty of liquids
Steam (e.g. showers or baths) to loosen secretions
Warm facial packs for 5-10 minutes 3-4 times a day to promote drainage
Saline nasal spray or drops may provide some relieve
Adequate rest
Elevate head of bed to promote sinus drainage
38. Medical therapy Acetaminophen or ibuprofen
Decongestants
Antihistamine
Mucoevacuants
Antibiotics
39. Antibiotics Amoxicillin remains as efficacious as newer drugs : 80-90 MKD divided bid for 10-14 days (maximum dose 2-3 g/day)
If not improvement : in 48-72 hrs ceftriaxone or amoxicillin-clavulanate 80-90 MKD divided bid for 7-10 days
Other treatment alternatives : cefdinir, cefpodoxime, cefuroxime
For severe allergies : azithromycin or clarithromycin
40. For the treatment of recurrent or chronic sinusitis, a more lengthy course of therapy, usually with a beta lactamase- resistant antibiotic, is desirable
3-4 week course of an appropriate antibiotic
In the immunocompromised patient, prophylactic antibiotic regimens are often utilized in addition to aggressive general management.
42. Surgical therapy Indirect sinus procedure
- septoplasty
- adenoidectomy
Direct sinus procedure
- antral lavage & sinus aspiration
- Nasal antral windows
- Middle meatal antrostomy
44. Complication Orbital involvement
- Preseptal cellulitis - Eyelid edema, erythema, normal globe movement
- Orbital cellulitis - Proptosis, chemosis
- Periorbital abscess - Proptosis with globe displaced inferolaterally, decreased extraocular muscle movement
- Orbital abscess - Severe proptosis, impaired visual acuity, fixed globe, toxic patient
- Cavernous sinus thrombosis - High fever, bilateral symptoms
45. Intracranial involvement
- Intracranial involvement usually occurs subsequent to direct spread from sphenoid or frontal sinus disease.
- Subdural and frontal lobe abscesses are most common.
-Meningitis may occur