Download
1 / 39
400 likes | 615 Views
STAMPEDE Systemic Therapy in Advancing or Metastatic Prostate cancer: Evaluation of Drug Efficacy. How to report Progressions and RT data. Sponsor number: MRC PR08 ISRCTN number: ISRCTN78818544 EUDRACT number: 2004-000193-31 CTA number: 00316/0026/001-0001.

E N D
STAMPEDESystemic Therapy in Advancing or Metastatic Prostate cancer: Evaluation of Drug Efficacy How to report Progressions and RT data Sponsor number: MRC PR08ISRCTN number: ISRCTN78818544EUDRACT number: 2004-000193-31CTA number: 00316/0026/001-0001
STAMPEDE uses multi-arm multi-stage methodology MAMS design permits rapid comparison and concurrent testing of treatments Currently using 1 investigational drug + research radiotherapy Issues in applying multi-arm multi-stage (MAMS)- methodology to a clinical trial in prostate cancer:the MRC STAMPEDE trial. M.Sydes et al., Trials.10. 39. http://www.trialsjournal.com/content/10/1/39 (Open access) Design rationale
Past accrual Possible future accrual Timelines: initial plans 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 A ADT-alone B ADT + zoledronic acid C ADT + docetaxel D ADT + celecoxib E ADT + zoledronic acid + docetaxel F ADT + zoledronic acid + celecoxib Follow-up
Past accrual Possible future accrual Accrual: end of Activity Stage II 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 A ADT-alone B ADT + zoledronic acid C ADT + docetaxel D ADT + celecoxib E ADT + zoledronic acid + docetaxel F ADT + zoledronic acid + celecoxib Follow-up
Past accrual Possible future accrual Timelines: from Nov-2011 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 A ADT-alone B ADT + zoledronic acid C ADT + docetaxel D ADT + celecoxib E ADT + zoledronic acid + docetaxel F ADT + zoledronic acid + celecoxib G ADT + abiraterone Follow-up
Past accrual Possible future accrual Timelines: from Jan-2013 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 A ADT-alone B ADT + zoledronic acid C ADT + docetaxel D ADT + celecoxib E ADT + zoledronic acid + docetaxel F ADT + zoledronic acid + celecoxib G ADT + abiraterone M1 only H ADT + RT Follow-up
Past accrual Possible future accrual Timelines: from March-2013 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 A ADT-alone B ADT + zoledronic acid C ADT + docetaxel D ADT + celecoxib E ADT + zoledronic acid + docetaxel F ADT + zoledronic acid + celecoxib G ADT + abiraterone M1 only H ADT + RT Follow-up
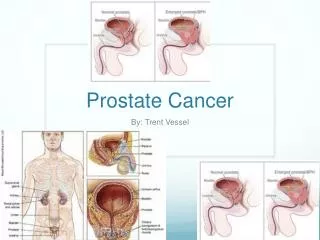
Four broad disease categories: Newly diagnosed high risk T3/4 N0 M0 Newly diagnosed node positive Tany N+ M0 Newly diagnosed metastatic TanyNany M+ Previously treated now relapsing: PSA 4ng/ml and rising with doubling time < 6 months PSA 20ng/ml N+ M+ Please see protocol section 4.1 and 4.2 for complete details about inclusion and exclusion criteria Main Inclusion Criteria
Follow-up dates will be sent to you on a treatment and follow-up schedule each time you randomise a patient. Please complete a follow-up form for each visit STAMPEDE Follow-up schedule
Types of progression: Biochemical Local Lymph node Distant metastatic Skeletal related event Each type of progression only needs to be reported once. Please complete an ‘additional treatmentupdateform’ if a patient receives additional treatment for a progression that you have already reported. Assessment of Treatment Failure
PSA Nadir Lowest reported PSA level Between randomisation and 24 weeks PSA Failure Depends on baseline PSA measurement and PSA nadir 3 possible PSA failure categories, A, B and C Defining PSA Nadir & PSA Failure Categories
3 PSA failure categories: PSA Failure Category A – When nadir is > 50% baseline (failed at time zero) PSA Failure Category B – Nadir is over 4ng/ml. Relapse occurs when PSA increases by 50% above nadir PSA Failure Category C – Nadir is under 4ng/ml. Relapse occurs when PSA increases by 50% above nadir or above 4ng/ml, whichever is greatest Defining PSA Relapse
Defining PSA Relapse • Ensure a confirmatory PSA test is done between 1 week and 3 months: • if value is ≥ PSA progression value then report biochemical progression • If the clinician decides that a patient has biochemically progressed before progression value is met (e.g. by adding anti-androgens): • Report progression as normal
Progression letters • PSA progression letters are sent out every 3 months for patients whom we have received their 24 week follow-up form Alternatively: • Please check appendix J for details of how to calculate the progression value OR • Contact the trial team for help
For M+ patients, treatment should continue until all progressions occur: PSA progression Radiological progression (appearance of new lesions or progression of existing lesions) Clinical progression (defined as new cancer-related symptoms) It is accepted that these flexible criteria for stopping treatment with abiraterone are open to the investigator’s interpretation and discretion. All progressions must be reported as per the other arms Assessment of Treatment Duration– Arm G
For N0M0 patients or N+M0 patients planned for RT treatment should continue until: 2 years or Disease progression as defined for M+ patients, whichever is sooner For patients with N+M0 disease not planned for radical radiotherapy should continue until: Disease progression as defined for M+ patients Assessment of Treatment Duration– Arm G
Reporting progressions on CRFs In case of progression, complete and return: • Follow up form for the relevant visit (e.g. week 6, 12, 18, 24 etc) • Progression and Additional Treatment form • End of treatment form (if applicable) • Death form (if applicable)
Reporting progressions on CRFs For patients on Arms A, B, C and E: • Please continue to follow up as normal and report data on Follow up (post-progression) form • Please ensure that any second-line treatments are reported on the form For patients on Arm G: • Please continue to follow up as normal but report data on Follow up form until all types of progression occur • Please ensure no further second-line treatment is given until: • all types of progressions are reported • trial abiraterone treatment is stopped
Some examples… Follow up form
Some examples… Progression and Additional Treatment Form
What to do post-progression • Continue to follow up patients as normal until death • Complete Follow up (Post-progression) form at each follow up visit • Ensure additional treatment post progression are reported using the Additional Treatments form • In case of missed follow up, please return the Follow up form as normal indicating • “Missed visit“ at the top of the form • PSA value (if known) • Week number
Standard-of-care radiotherapy N0M0 patients: Investigators should give radiotherapy (RT) to patients with N0M0 disease, in accordance with the recent data from the PR07 and SPCG trials If there is an intention to omit radiotherapy in patients with N0M0 disease this must be discussed with the MRC CTU before consent N+M0 patients: the benefit of radiotherapy in this group is at present uncertain. Investigators will be asked to state their intention with regard to planned radiotherapy in this group at randomisation RT given 6 to 9 months after randomisation
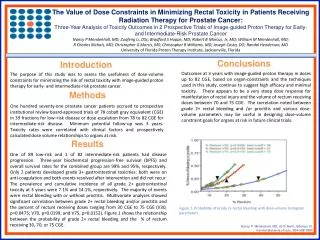
The use of radiotherapy to the prostate will retard progression of the metastases in men presenting with metastatic prostate cancer The primary tumour may be required to stimulate disseminated tumour cells to grow into metastases Supporting evidence in renal and prostate cancer (SWOG 8949, EORTC 30947, MRC PR07 /NCIC PR.3 trials) Research (M1) Prostate Radiotherapy
For patients who receive a primary or research course of radiotherapy, complete and return Radiotherapy detail form Radiotherapy acute toxicity form For patients who receive a palliative course of radiotherapy, complete and return Palliative radiotherapy form Reporting radiotherapy data
Reporting radiotherapy data • For patients who receive RT, RT detail form should be completed when the patient's course is completed • For standard-of-care RT, please ensure forms are completed and returned after a maximum of 12 months post-randomisation • For research (M1) RT to prostate please ensure forms are completed and returned after a maximum of 8 weeks post-randomisation • For patients who do not receive primary RT, it should be completed 10 months after randomisation to confirm that RT was not given
Some examples… RT detail form
Some examples… RT acute toxicity form
Conclusion • Ensure Failure Free Survival events (e.g biochemical progression) is reported appropriately • Arm-specific rules • Treatment duration • Follow up continues until death (overall survival) • Report RT information: • Standard-of-care RT (M0N0 or M0N+) • Research RT to prostate (newly diagnosed M+)
Nick James Oncologist; CI, Chair, Birmingham, UK Noel Clarke Urologist; Vice-Chair Manchester, UK Malcolm Mason Oncologist; Vice-Chair Cardiff, UK Alastair Ritchie Trial Surgeon MRC CTU David Dearnaley Oncologist Sutton, UK Chris Parker Oncologist Sutton, UK Robert Millman Patient representative Stockport, UK John Masters Pathologist London, UK Martin Russell Oncologist Glasgow, UK Marc Schulper Health Economist York, UK Andrew Stanley Pharmacist Birmingham, UK George Thalmann Oncologist Bern, CH Daniel Aebersold Clinical Oncologist Bern, CH Estelle Cassoly Trial Coordinator SAKK, CH Claire Amos Clinical Project Manager MRC CTU, UK Francesca Schiavone Clinical Trial Manager MRC CTU, UK Alanna Brown Clinical Trial Manager MRC CTU, UK Dominic Hague Data Manager MRC CTU, UK Katie Ward Data Manager MRC CTU, UK Peter Vaughan Data Manager MRC CTU, UK Melissa Spears Trial Statistician MRC CTU, UK Max Parmar CTU Director MRC CTU, UK Matthew Sydes CTU Lead/Senior Trial Statistician MRC CTU, UK Trial Management Group
Contact us Web: www.stampedetrial.org MRC Francesca Schiavone Clinical Trial Manager T: +44 (0) 207 670 4632 E: mrcctu.stampede@ucl.ac.uk Alanna Brown Clinical Trial Manager T: +44 (0) 207 670 4882 E: mrcctu.stampede@ucl.ac.uk Dominic Hague, Katie Ward, Peter Vaughan STAMPEDE Data Managers T: +44 (0) 207 670 4809 / 4794 / 4947 E: mrcctu.stampede@ucl.ac.uk