Download
1 / 75
780 likes | 1.18k Views
Systemic Lupus Erythematosus, ANA’s, etc. Hermine Brunner, MD MSc Assistant Professor of Pediatrics Division of Rheumatology Cincinnati Children’s Hospital Medical Center. SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)- DEFINITION/DIAGNOSIS. Prototype of auto-immune, multi-system disease

E N D
Systemic Lupus Erythematosus, ANA’s, etc. Hermine Brunner, MD MSc Assistant Professor of Pediatrics Division of Rheumatology Cincinnati Children’s Hospital Medical Center
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)- DEFINITION/DIAGNOSIS • Prototype of auto-immune, multi-system disease • Onset maybe acute, episodic, or insidious • “Anything” can happen to “any organ system” • Antinuclear antibodies are almost always present • Serositis & Immune complexes
SLE - EPIDEMIOLOGY • 20% of all SLE is pediatric age group • Incidence 0.6/100,000 • Prevalence 5-10/100,000 • Overall 5-10,000 children in U.S.A. • Approximately 5% of new diagnoses in Pediatric Rheumatology clinics • SLE : JRA/1:10 ratio
Pediatric SLE versus Adult Onset SLE • More severe symptoms at onset • More aggressive clinical course than adults • Increased need for corticosteroid; 77% vs 16% • Children tend to die during acute SLE phase Adults tend to die secondary to complications • African American and Hispanic children have a higher incidence of disease • African American patients have • higher prevalence and severity of renal • higher prevalence neuropsychiatric SLE • higher titers of anti-DNA and anti-SSA antibodies in association with cardiac disease
Genetics in SLE • Eight of the best supported SLE susceptibility loci are the following • 1q23 • 1q25-31 • 1q41-42 • 2q35-37 • 4p16-15.2 • 6p11-21 • 12p24 • 16q12 Tsao, BP, Curr Opinion Rheum, 2004; 16: 513-521
THE 1982 REVISED CRITERIA FOR CLASSIFICATION OF SLE Malar rash Serositis Discoid rash Renal disorder Photosensitivity Neurologic disorder Oral ulcers Hematologic disorder Arthritis Immunologic disorder Antinuclear antibody Revised 1997
THE 1982 REVISED CRITERIA FOR CLASSIFICATION OF SLE • For the purpose of identifying patients in clinical studies, a person shall be said to have SLE if any 4 or more of the 11 criteria are present, serially or simultaneously, during any interval of observation. • Sensitivity 96% • Specificity 96% in adults • Similar percentages in pediatric group.
MALAR RASH • Fixed erythema, flat or raised, over the malar eminences • tending to spare the nasolabial folds
DISCOID RASH • Erythematous raised patches with adherent keratotic scaling and follicular plugging; • Atrophic scarring may occur in older lesions
PHOTOSENSITIVITY • Skin rash as a result of unusual reaction to sunlight • by patient history or physician observation
ORAL ULCERS • Oral or nasopharyngeal ulceration • Usually painless, observed by a physician
ARTHRITIS • Nonerosive arthritis involving 2 or more peripheral joints • Characterized by tenderness, swelling, or joint effusion.
SEROSITIS A) Pleuritis - convincing history of pleuritic pain or rub heard by a physician or evidence of pleural effusion OR B) Pericarditis - documented by ECG or rub or evidence of pericardial effusion
RENAL DISORDER A) Persistent proteinuria greater than 0.5 grams per day or greater than 3+ if quantitation not performed OR B) Cellular casts - may be red cell,hemoglobin, granular, tubular, or mixed
NEUROLOGIC DISORDER A) Seizures - in the absence of offending drugs or known metabolic derangements, e.g., uremia, ketoacidosis, or electrolyte imbalance OR B) Psychosis - in the absence of offending drugs or known metabolic derangements, e.g. uremia, ketoacidosis, or electrolyte imbalance
HEMATOLOGIC DISORDER A) Hemolytic anemia - with reticulocytosis OR B) Leukopenia - less than 4,000/mm3 total on 2 or more occasions OR C) Lymphopenia - less than 1,500/mm3 on 2 or more occasions OR D) Thrombocytopenia - less than 100,000/mm3 in the absence of offending drugs
IMMUNOLOGICDISORDER A) Anti-dsDNA: antibody to native DNA in abnormal titer OR B) Anti-Sm: presence of antibody to Sm nuclear antigen OR C) Antiphospholipid antibodies by positive IgG or IgM anticardiolipin antibodies or positive test for lupus anticoagulant
ANTINUCLEAR ANTIBODY • An abnormal titer of antinuclear antibody by immunofluorescence or an equivalent assay • at any point in time • and in the absence of drugs known to be associated with • “drug-induced lupus” syndrome
Drug-Induced Lupus • Minocycline (Minocin) • Phenytoin (Dilantin) • Carbamazepine (Tegretol) • Ethosuximide (Zarontin)
ANTINUCLEAR ANTIBODY • 1:20 - 1:40 Screening titer • 1: x titer • Pattern • speckled - + ENA’s • rim - ds DNA • homogeneous - DNA (LE prep) • nucleolar - Scl - 70
SLE Tissue Specific Nuclear Antibodies Antibodies ATA Ro/SSA Anti ASMA La/SSB Anti-MITO RNP Anti-LKM Sm Anti-PC ds DNA Hep-2 ss DNA
Arthralgia and Positive ANA or RF • Remember that objective signs of joint inflammation substantiate diagnosis of arthritis • Comprehensive review of systems may uncover clues • Perform a critical, complete physical examination • Serial re-evaluations may be necessary • Most children do not progress to a C.T.D. • Positive serologies may be seen in: • Normal children - approximately 3-12% • Response to infection
Persistent ANA • 24/108 children with musculoskeletal problems had positive ANA • 21/24 had persistent ANA, mean duration 38 mo • No patient developed an overt autoimmune or inflammatory disease, mean F/U 61 mo (13-138) • Conclusion: a child with positive ANA and musculoskeletal problems , but with no evidence at presentation of AID or inflammatory disease is at low risk of developing such a disease. Cabral, DA, et al Pediatrics 1992, 89(3):441-444
Outcome of Children referred to Pediatric Rheumatology Clinic with a positive ANA but without AID • 500 new patients reviewed, 113 had positive ANA • 72 (64%) had an autoimmune disease AID, 10 (9%) were lost to F/U, 31 (27%) had no AID, • Mean ANA titer 1:160, varied pattern • Mean clinical F/U 37 mos • 25 (81%) cleared their symptoms, 5 (16%) had improvement, 1 developed autoimmune hepatitis • Prognosis with +ANA is excellent in absence of AID at presentation Deane, PMG, et al, Pediatrics 1995, 95:892-895
Clinical Utility of Antinuclear ANA Tests in ChildrenMcGhee JL et al, BMC Pediatrics 2004, 4: 13 • 110 pts referred to Rheum for +ANA • 80 children with musculoskeletal problems syndromes • 10 pts subsequently dx’d SLE, 1 MCTD, 1 Prim Raynaud’s, 18 with JIA • Nonurticarial rash more common in SLE, p=0.007 • Children with SLE were older 14.2 vs 11 yrs, p=0.001 • ANA > 1:640 was +predictor for SLE while titers of <1:360 were negative predictors • Conclusion: • Age and ANA titer assist in Dx SLE, no diagnostic value in Dx JRA • Remember the AID have objective evidence of disease!!!!!!!
SLE - CLINICAL MANIFESTATIONS Most common signs/symptoms • Unexplained fever, any pattern • Malaise • Weight Loss • Arthralgia
SLE - MUCOCUTANEOUS INVOLVEMENT • “Butterfly Rash” - 1/3 at onset • Angiitic papules • Periungual erythema • Urticaria / angioedema • Palatal ulcer / aphthous ulcer • Alopecia
SLE - MUCOCUTANEOUS INVOLVEMENT • Discoid lupus • Subacute cutaneous lupus • Livedo reticularis • Nailfold capillary changes • Vasculitic ulceration • Panniculitis • Nasal septal perforation
Ulcerated leukocytoclastic vasculitis in SLE
SLE - MUSCULOSKELETAL DISEASE • Arthralgia / Arthritis • Myalgia / Myositis • Ischemic necrosis of bone - AVN
SLE - VASCULOPATHY • Small vessel vasculitis • Palpable purpura • Raynaud’s phenomenon • Antiphospholipid antibody syndrome
SLE - CARDIAC INVOLVEMENT • Pericarditis • Myocarditis • Endocarditis, Libman-Sacks • Accelerated atherosclerosis
SLE - PLEUROPULMONARY DISEASE • Pleuritis/Pleural effusion • Infiltrates/Atelectasis • Acute lupus pneumonitis • Pulmonary hemorrhage • “Shrinking lung” - diaphragm dysfunction • Subclinical restrictive disease
SLE - GASTROINTESTINAL MANIFESTATIONS • Anorexia, weight loss, nonspecific abdominal pain • Pancreatitis • Mesenteric arteritis • Esophageal dysmotility
SLE – LIVER , SPLEEN & LYMPH NODE • Generalized lymphadenopathy • “Lupoid hepatitis” vs SLE hepatic involvement • Functional asplenia
SLE - NEUROPSYCHIATRIC MANIFESTATIONS • Must be differentiated from infection or hypertensive or metabolic complications • Any level of the CNS/PNS can be affected • Thorough evaluation necessary - CSF, EEG, CT, MRI, EMG / NCV, NP testing
SLE - NEUROPSYCHIATRIC INVOLVEMENT Behavior/Personality changes, depression Cognitive dysfunction Psychosis Seizures Stroke Chorea Pseudotumor cerebri Transverse myelitis Peripheral neuropathy Total of 19 manifestations described
SLE - RENAL INVOLVEMENT • Usually asymptomatic • Gross hematuria • Nephrotic syndrome • Acute renal failure • Hypertension • End stage renal failure
SLE - NEPHRITIS Nephritis remains the most frequent cause of disease-related death.
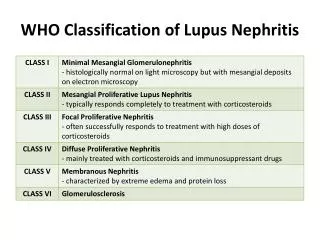
WORLD HEALTH ORGANIZATION CLASSIFICATION OF LUPUS NEPHRITIS Class I Normal Class II Mesangial IIA Minimal alteration IIB Mesangial glomerulitis Class III Focal and segmental proliferative glomerulonephritis Class IV Diffuse proliferative glomerulonephritis Class V Membranous glomerulonephritis Class VI Glomerular sclerosis
SLE - LABORATORY EVALUATION • Antinuclear antibody profile • Anti dsDNA abs, Sm abs • C3, C4, IgA, IgG, IgM • Direct Coomb’s, DAT • Antiphospholipid antibodies ACLA - Anticardiolipin antibodies LAC - Lupus anticoagulant • CBC with Diff, U/A, CMP, TSH, ESR
Comprehensive Evaluation of a Child with SLE • Cumulative medication burden • Serial DEXA while on corticosteroids • Lipid panels • Repeat APA profile, ? Frequency • HRQL and damage indices, SLEDAI, SDI • Neuropsychiatric testing ? • ECHO • Complement factor deficiency (C1q)
Long-term Management Issues • Long term morbidity of corticosteroids: short stature, cataracts, osteoporosis • How to manage ongoing active disease after multiple medications during childhood • Long term morbidity of immunosuppressive agents • Non-sustained durable disease: ? remission • Cumulative risk re: malignancy and premature ovarian failure
Therapeutic Goals in SLE: Still Unmet Expectations • Rate of renal remission after first line therapy still 81% at best • Renal relapse in 1/3 pts mostly still immunosuppressed • 5- 20% experience ESRD 5-10 yrs after disease onset • Treatment related toxicity remains a concern; osteoporosis, premature ovarian failure, severe infections, etc. • Prognostic factors have been identified but are difficult to modify in order to improve outcomes
Treatment Regimens for LN • Glucocorticoids plus cyclophosphamideinduction & maintenance for 3 years • NIH protocol • Glucocorticoids plus low dose cyclophosphamide with maintenance with MMF or AZA • Immunoablative doses of cyclophosphamide • Autologous stem cell transplantation • Plasmapharesis is not recommended • Reviewed: Houssian FA, J Am Soc Nephrol 2004; 15: 2694
Sequential Therapies for WHO III- V • 60 adult SLE pts randomized 3 groups • 12 Class III, 46 Class IV and 1 Class Vb • All received initial therapy with Cyclophosphamide 0.5-1.0 gm/m² up to 7 pulses • Cont’d on 1) cyclophosphamide, 2) azathioprine 1-3mg/kg, or 3)M ycophenolate mofetil (Cellcept, MMF) 0.5-3.0 gm/d for 1-3 years • 5 pts died- 4CYC, 1 MMF; 5 CRF- 3 CYC,1 AZA, 1 MMF • 72 month event free survival rate higher in MMF and AZA than in CYC (P=0.05 and P=0.009, respectively) • Incidence of hosp, amenorrhea, infections, nausea and vomiting lower in the MMF and AZA groups than in the CYC group Contreras, G et al: NEJM 350(10): 971-980, 2004