Download
1 / 31
310 likes | 324 Views
Addressing depression in Muslim communities: development of a treatment manual for professionals. Ghazala Mir Shaista Meer Dean McMillan, David Cottrell, Allan House. Leeds Institute of Health Sciences NHS Bradford and Airedale, Bradford District Care Trust

E N D
Addressing depression in Muslim communities:development of a treatment manual for professionals Ghazala Mir Shaista Meer Dean McMillan, David Cottrell, Allan House Leeds Institute of Health Sciences NHS Bradford and Airedale, Bradford District Care Trust Sharing Voices Bradford, University of York
Background: religion, therapy and coping • Culturally appropriate treatment - promoted by NICE and Department of Health • People from Muslim backgrounds - more likely to use religious coping techniques for mental illness than other faith groups in the UK • Faith-sensitive therapies - potential to reduce levels of depression and improve wellbeing • Behavioural Activation - proven effective in clinical trials. Focus on client values promising for adaptation to meet the needs of Muslim clients.
Aims • Fill current gaps in knowledge about how to address the needs of Muslim service users with depression. • Develop a faith-sensitive therapy for Muslim service users • Test across diverse groups within Muslim communities • Capacity for testing adaptations across interventions for other kinds of mental disorder.
Plan of investigation Four phases broadly follow MRC guidelines for development of complex interventions: • PHASE 1: Synthesis of literature • PHASE 2: Interviews with key informants PHASE 3: Synthesis and production of treatment manual • PHASE 4: Piloting.
Evidence from existing literature Potential adaptations and mechanisms by which these could influence outcomes: • Therapy models and interventions (including BA) involving any religion/ spirituality • For Muslim clients with depression: • Influences on healthcare and mental health • Strategies for engaging effectively • Faith-based coping strategies • Diversity between and within Muslim communities (eg gender/ ethnicity/religiosity/age) • Similarities/differences with other social groups.
Literature: existing evidence • KI interviews: service users and practitioners (GPs/clinical psychologists/ service managers/community groups) • Three advisory groups: advice from professionals and service users, Muslim service users and a virtual expert group • Pilot: therapists, clients, supervisors, and managers interviewed Synthesis
Themes used for synthesis: • Spiritual understandings of health • Consistency with cultural values and beliefs • Client –therapist match • Easily accessible interventions • Strategies to use the family • Sensitivity to support and resources available, (eg friends, community organisations) • Social context
Spiritual understandings of health RELIGION AND THERAPY • Positive religious coping: resilience, hope, making sense of experience, increased self-esteem • Negative religious coping: punishment, obsessive behaviour, guilt, despair, hopelessness encourage valued religious activity without inducing guilt • “Islamic way of life” = good health; • Islamic scriptures support healing and link values/beliefs with actions. range of religious teachings a resource for improving health ISLAM AND HEALTH
Cultural values and beliefs • Norms and values from non-scriptural sources • Can be oppressive towards some members of Muslim communities (eg young people/women) • Intertwined with religious beliefs - may be supported by biased interpretations of teachings eg emphasising rights of dominant family members • Can be challenged through religious teachings/ alternative interpretations • Involvement of someone with knowledge of Islamic teachings can help clarify /empower those less powerful
Client-therapist match • Therapist’s background not primary concern: understanding/openness, protection of professional boundaries, compassionate/ non-judgemental approach • Shared background: shared understanding, less need to explain/justify, empathy but fears re confidentiality, judgemental approach and crossing professional boundaries • Non-shared background: less fear of being judged/no concerns around confidentiality– but poor engagement with religious identity, stereotyping, inappropriate curiosity • Knowledge/interest in Islam: message of social inclusion. Need for therapist self-reflection on attitudes towards religion/Islam/preconceived ideas.
Religious activation: Client Self Help Booklet • Collection of teachings from the Qur’an/Sunnah. • Resource for both the therapist and the client • Teachings linked to positive religious coping and principles of BA • Content guided by clinical psychologist qualified in Islamic jurisprudence • Booklet includes action points and space for reflection
BA approach: Islamic teachings • BA approach Being active • Client booklet “Tie your camel” “Prophet Muhammad (pbuh) noticed a Bedouin leaving his camel without tying it. He asked, "Why don't you tie down your camel?" The Bedouin answered, "I put my trust in Allah." The Prophet said, "Tie your camel first, then put your trust in Allah"
BA approach: Islamic teachings • BA approach Achievable goals • Client booklet One step at a time • The Prophet, (pbuh) was asked: 'Which deed is most beloved to Allah?' He said, ' The one that is done regularly, even if it is little.’
Manual flexibility BA-focus Islam-focus Intervention will always be 100% BA
Manual flexibility BA-focus Islam-focus For some people, a focus on Islam will not be relevant
Manual flexibility BA-focus Islam-focus For others it will be very relevant
Manual flexibility BA-focus Islam-focus May be somewhat relevant for others Yet others may feel ambivalent towards religion
Family and social support/social context • Family involvement encouraged eg to support access, homework tasks, family understanding – client choice, may need therapist support • Collaboration with community organisations/ experts encouraged – need for more research • Activation to address social context of Muslims in UK eg unemployment, poor health, social exclusion • Therapist strategies to encourage session attendance/prevent early withdrawal
Pilot aims • Train therapists from diverse ethnic, religious and gender backgrounds. • Recruit 20 adult Muslim patients with depression: diversity in gender, language and age. • Deliver intervention in BDCT via range of practitioners eg Psychological Wellbeing Practitioners (PWP) and clinical psychologists.
Delivery: Pilot process • Ten therapists trained to deliver intervention - dropout due to sickness (2) left work (3) other commitments (1), unwillingness to deliver intervention (1) 2 therapists delivered intervention fully; one partial involvement (sick leave). • +Four month delay in participant recruitment: problems with consent process and team or management support for recruitment
Pilot process Participants: • 19 participants recruited; 14♀ 5♂, aged between 23-56. • Mainly British Pakistani backgrounds (n=17). • 9 service users received therapy in English and 9 in Urdu or Mirpuri, 1 service user spoke Hindko. Intervention: • Manual based on up to 12 sessions x 1 hour • Therapy impact: qualitative interviews + PHQ9, GAD7 (routine IAPT measures) and WSAS • Sessions recorded to check for therapist adherence to the manual. • Bi-monthly peer supervision sessions – facilitated by Jonathan Kanter via weblink in addition to routine supervision
Evaluation of therapy: Pilot evaluation • Adherence to manual checked independently by 2 members of research team. • Qualitative interviews – 13 service users and 15 professionals (therapists, supervisors and team managers) interviewed: • 7 service users who completed + 6 who withdrew/stepped up • 7 therapists (including 5 trained but didn’t deliver) • 1 therapist working outside study • 5 supervisors • 2 team managers • Statistical analysis of PHQ-9 scores
Findings • Adherence: therapists on whole delivered BA but did not always pick up on religious issues. • BA: Most service users positive about focus on behaviour Therapists attitudes more varied – eg BA not always seen as relevant for complex depression and relationship problems/more guidance on how to deal with thoughts • Religion: Service users confirmed importance of religion/ positive about therapy drawing on religious values; therapists recognised that helpful approach for some service users, but could still struggle with how to put it into practice.
Findings • Some service users preferred a Muslim therapist; most said it was not necessary provided the therapist could support working with their values. • Service users and therapists felt some level of knowledge about Islam was important. Some therapists wanted link to someone who could advise on Islam. • Therapists who delivered the intervention felt confidence to work with religious beliefs grew with practice. • Values assessment: very important for some clients but not usual practice for PWPs, linked to higher level training
Findings • Client booklet: service users very positive on the whole but wanted more link with the therapy. Therapists demonstrated some lack of understanding of its function and at times gave out without adequate explanation. • Community resources: therapists didn’t feel it was their role to build links, however some service users said that they would have found these useful e.g. checking out questions about prayer with an imam • Possible under referral of Muslim service users for therapy, particularly those who do not speak English – low GP referrals and stigma of mental health services suggested; service users suggested offering intervention in community settings
Findings: Findings • Impact of therapy: almost all service users positive, for some seen as a stepping stone to recovery. • Withdrawal – Follow up/discharge procedures in manual not usually followed because of time pressures on therapists. Reasons for withdrawal: wanted therapist to focus more on religion (1) or thoughts (1), session times clashed with social group (1), therapy provided closure (1), wanted to deal with problems in family first (1), busy/didn’t feel benefit (2). • Stepping-up: more client negotiation/consideration of BA effectiveness needed • Training: more detail needed on Values Assessment, using the client booklet, working with unhelpful thoughts, working with families and community resources
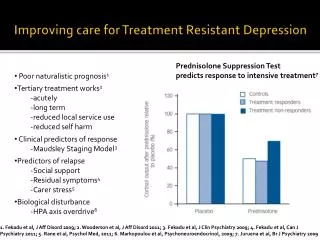
Depression measures • Acceptable to clients and resonated with their experience • Not always completed, especially translated versions • 35% of 108 possible measures missing • change in PHQ scores for 14 clients using initial and final scores . Reliable change as 5 or more points; clinically significant improvement as move from 10 or above pre-treatment to 9 or below at post-treatment : • 4 increased final PHQ scores: 1 increased by 5 points • 10 decreased scores: 4 reduced by 5 or more. One with clinically significant improvement from 14 pre-treatment to 4 post-treatment • Considerable caution needed for these results given the absence of a control group.
Recommendations - Implications for services Conclusion • Intervention is acceptable to most clients and therapists and feasible in practice • Therapist training needed on values assessments, working with families and working with community organisations/resources • Access to expertise in BA/knowledge of Islam needed to reduce withdrawal from therapy • Placing services in community settings may decrease stigma, increase referrals and improve access to services.
Recommendations - research: Conclusion • Study confirms importance of exploring and working with client religious beliefs in therapy. • Strategy for improving recruitment developed through lessons from pilot study • Whole team approach likely to be more successful than with individual therapists • Wider range of recruitment sources • Support for consent process • Further research on effectiveness of enhanced BA possible – currently seeking interested sites
Ghazala Mir: g.mir@leeds.ac.uk Shaista Meer: s.m.meer@leeds.ac.uk Leeds Institute of Health Sciences University of Leeds Charles Thackrah Building 101 Clarendon Road Leeds, United Kingdom LS2 9LJwww.leeds.ac.uk/lihs This presentation presents independent research commissioned by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-1208-18107). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health