Download
1 / 49
550 likes | 1.1k Views
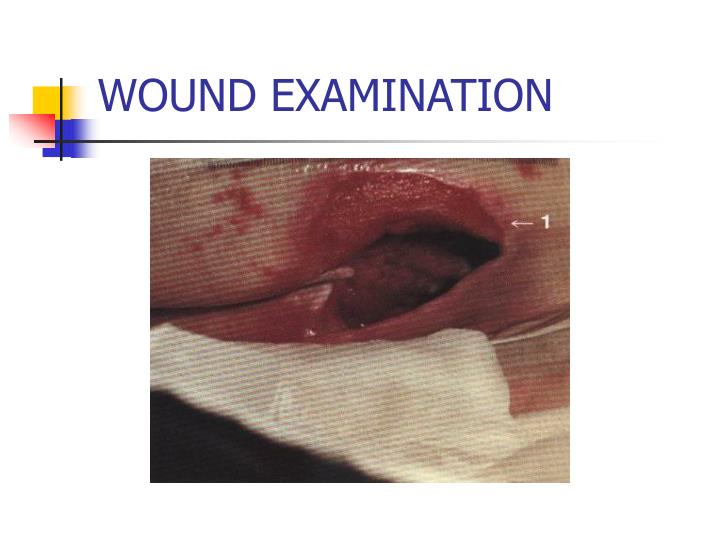
WOUND EXAMINATION. PATIENT HISTORY. WOUND HISTORY DURATION ATTRIBUTING EVENT SYMPTOMS PAIN PARESTHESIA/ANESTHESIA. HISTORY (cont.). DOES PAIN CHANGE WITH POSITION elevation decreases pain = venous dependency increases pain in venous lesions pain with rest - severe occlusive disease

E N D
PATIENT HISTORY • WOUND HISTORY • DURATION • ATTRIBUTING EVENT • SYMPTOMS • PAIN • PARESTHESIA/ANESTHESIA
HISTORY (cont.) • DOES PAIN CHANGE WITH POSITION • elevation decreases pain = venous • dependency increases pain in venous lesions • pain with rest - severe occlusive disease • intermittent pain with ambulation = claudication
HISTORY (CONT.) • PRES.MH, PMH, PSH (PVD, CHF, HTN, DM, THYROID, LYMPHEDEMA, IMMUNOSUPPRESSIVE, CA , R/A ETC.) • PAST TREATMENT & OUTCOME • MEDICATIONS • TESTS (CULTURES, DOPPLERS, BONE SCAN, X-RAY)
HISTORY (CONT.) • ADDITIONAL STUDIES (ARTERIOGRAM, VENOGRAM, ABI) • SOCIAL HX • VOCATIONAL HISTORY • HOBBIES
OBJECTIVE EVALUATION • Test & Measures
LOCATION • HYPERTENSIVE-posterio/lateral leg, onset with infarction, very severe pain hypertension • VENOUS-distal leg, medial aspect, red base, wet, periwound skin staining, no pain, mild insufficiency
Chronic Venous Insufficiency: “champagne bottle” “piano leg” appearance Atrophie blanche
LOCATION (CONT.) • ARTERIAL-DISTAL LOWER EXREMITY, LATERAL ASPECT, TOES & FEET, PALE BASE, ATROPHIC SKIN, DRY WOUND, SEVERE PAIN, ARTERIOSCLEROSIS • NEUROTROPHIC-PLANTAR SURFACE OF FOOT, SMALL OR DEEP, PERIWOUND CALLOUS, INFECTION, NO PAIN POSSIBLE DM
SIZE • LENGTH, WIDTH, AREA, DEPTH, VOLUME - IF REMOVE ESCHAR WOUND WILL APPEAR BIGGER • MEASURE FROM WOUND EDGE • USE CONSISTENT TOOL & UNITS OF MEASUREMENT • PHOTOGRAPHY, TRACING, VOLUME, SYRINGE
UNDERMINING • ALSO KNOWN AS RIMMING OR TUNNELING • TISSUE DESTRUCTION UNDERLYING INTACT SKIN ALONG THE WOUND MARGINS (HYPOGRANULATION) • MEASURE USING THE O’CLOCK SYSTEM, HEMISPHERES
GIRTH • EDEMA, ATROPHY • MEASURE WITH REFERENCE TO BONY LANDMARKS USING TAPE MEASURE • VOLUMETRIC DISPLACEMENT
Edema • Measured in a variety of ways: • Quantifying Pitting that occurs from the examiner’s digit • 1+ Barely perceptible depression • 2+ Easily identified depression, 15 sec. to resolve • 3+ Depression takes between 15-30 sec. to resolve • 4+ Depression lasts for greater than 30 sec.
SHAPE • TRIANGULAR- SKIN TEAR • ROUND- ARTERIAL • IRREGULAR-VENOUS
SLOPES • ANGLES OF MARGINATION • DEPICT GRANULATION • VERY IMPORTANT MEASUREMENT
Staging of Wounds • Stage I-IV Pressure Wounds • Wounds other than Pressure • Superficial • Partial Thickness -epidermal layer, superficial layer of dermis • Full-Thickness- epidermis, dermis, subcutaneous , may also involve muscle and bone
Stage I • Partial Thickness, limited to epidermis, non-blanchable erythema (sunburn)
Stage II • Partial Thickness Skin Loss, • involves both epidermis and dermis • (abrasion, blister, shallow crater)
Stage III • Full Thickness Skin Loss • Damage or Necrosis of Subcutaneous Tissue • May Extend to Fascia • (deep crater, with or without undermining)
Stage IV • Full-Thickness Skin Loss • Extensive Destruction • Necrosis • Damage to Muscle, Tendon, Joint Capsule, Bone
Wagner Ulcer Classification Diabetic Ulcers • Grade • 0 Intact Skin • 1 Superficial Ulcer • 2 Deep Ulcer • 3 Deep Infected Ulcer • 4 Partial Foot Gangrene • 5 Full Foot Gangrene
Tissue Composition • RED WOUNDS- clean healthy granulating wounds • YELLOW WOUNDS-may contain fibrous tissue, hydrated necrotic tissue, or dead tissue, referred to as slough • BLACK WOUNDS-dried eschar, leathery
Tissue Found in Wounds • Eschar • Granulation • Adipose • Fascia • Muscle • Tendon • Bone
Foreign Debris & Necrotic Tissue • Remove as Soon as Possible • This will prevent bacterial colonization and infection
Peri-Wound • Trophic Changes (dry skin, brittle nails, hair loss) • indicates poor arterial nutrition
Peri-Wound • Change in skin color • cyanotic = Arterial Compromise • Pigmentation (hemosiderin staining), pigment is deposited from RBC = Venous • Ring of Redness or Halo of erythema around the wound may indicate infection
Drainage • Inactive • found on dressing, at time of observation no drainage is found in or near the wound
Drainage • Active • Free flowing, able to be milked from the wound
Characteristics of Drainage • Transudate (Serous): clear, watery • contains: H20, salts and proteins • Serosanguineous: tinged red/brown • watery, thin • contains: serum, blood • Exudate: creamy, yellowish • moderately thick • contains: proteins, WBC
Characteristics of Drainage (cont.) • Purulent/Pus: yellowish/brownish • Thick • contains: WBC, necrotic debris • Infected Pus • yellow, green/blue • thick • contains: pathogens • describe amount:none, min, mod, max
Odor • Pseudomonas-sweet smell (fruity) • Garbage- rotten= infection • Proteus- ammonia • describe; absent, mild, moderate, foul smelling
Temperature • systemic v. localized • measured • touch • thermistor • thermography • radiometer • measure infrared radiation from the body
Indications for culture • Clinical Signs of Local Infection by Linholm • edema, erythema, purulent or foul smelling drainage, increased pain, induration, heat around the wound; IFEE • Signs of systemic infection • fever, abnormal CBC • Bone Involvement (osteomyelitis) • Non-Healing Wounds (silent infection)
Aerobic swab culture technique. The culturette Is rotated while moving in a 10-point pattern. Gentle pressure to express fluid is required. From: Myers, B.A. Wound Management: Principles and Practice. Prentice Hall, Upper Saddle River, NJ. 2004: p. 94
Vasculature Examinations • Pulses(2+Normal, 1+Diminished, 0 Absent) • Auscultation (swishing sound, only heard in abnormal artery) • Venous Exam (venous doppler)
Vascular Exams Continued • arterial exam • ankle-brachial index (ABI) • sys.pres.LE/sys.preUE (120/100=1.2 normal) • should equal 1 or greater than 1 • 1 or greater = no arterial occlusive disease • 0.9-1.0 minimal symptoms in LE • 0.5-0.9 claudication pain • 0.3-0.5 ischemic rest pain • less than 0.3 ischemia with tissue necrosis
Normal ABI Ankle SBP 120mmHg Heart Level SBP 100 mmHg ABI 120 mmHg/100mmHg= 1.2 Doppler Doppler
ABI • When ABI value is <.9 • 95% sensitive • 99% specific • For angiographically significant PVD
ABI • Change of 0.15 correlates with disease and symptomology
Tissue Oxygen Tension • tc-Po2 • transcutaneous oximmetry
Rubor of Dependency Test • assess arterial flow by evaluating skin color changes during elevation and dependency • leg elevation at 60 degrees for 1 min. • normally no significant change in color • lower the leg, record time for color return • arterial insufficiency may take longer than 30 sec. • color will be bright red (hyperemic)
VENOUS FILLING TIME • assess arterial flow by evaluating time veins take to fill after emptying • elevate LE for 1 min. to 60 degrees • lower the leg, record time that veins on the dorsum of the foot take to refill • with arterial insufficiency may take 30 sec. or longer
Claudication Time • assess arterial response by increasing the demand to the calf musculature during exercise • Treadmill- 1-2MPH • measure time to claudication • monitor changes in functional status over time
Test for DVT • Homan’s Sign • squeeze calf while dorsiflexing the ankle, with the knee held in an extended position • tenderness with increased firmness may suggest DVT • confirm using blood pressure cuff • pt. unable to tolerate 40mmHg if DVT present • normally able to tolerate much higher pressures
Test for Cutaneous Sensitivity • perception of light touch • use cotton ball • perception to temperature • warm, cool • 2-point discrimination
Monofilament Testing for LOPS • Semmes-Weinstein Monofilaments • Scale of 1.65 to 6.65 -- force required to cause the filament to bow when pressed against the skin • Higher the monofilament number, the more force required for bending. • Diabetes– Standard of examination • 5.07 monofilament, on bowing exerts 10g of force