Download
1 / 7
70 likes | 229 Views
ASTHMA 2009. RAMESH KAUL, MD M Surgery FCCP. Asthma definition. Asthma: Definition by WHO

E N D
ASTHMA 2009 RAMESH KAUL, MD M Surgery FCCP
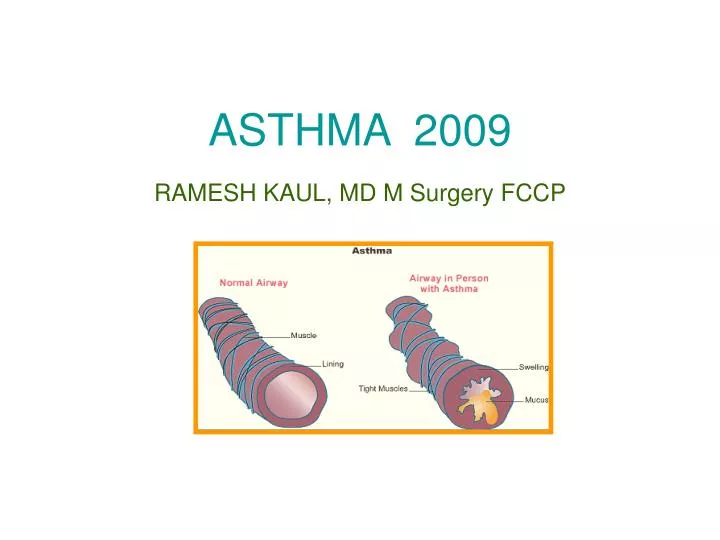
Asthma definition • Asthma: Definition by WHO • Asthma attacks all age groups but often starts in childhood. It is a disease characterized by recurrent attacks of breathlessness and wheezing, which vary in severity and frequency from person to person. In an individual, they may occur from hour to hour and day to day. • This condition is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they become easily irritated. In an attack, the lining of the passages swell causing the airways to narrow and reducing the flow of air in and out of the lungs.
Asthma epidemiology • According to WHO estimates, 300 million people suffer from asthma and 255 000 people died of asthma in 2005. Asthma is the most common chronic disease among children. • Children, boys , blacks and women have higher prevalence
Asthma Severity staging of disease Mild Intermittent Symptoms<2 times a weeksAsymptomatic and normal PEF between exacerbationsExacerbations brief (from a few hours to a few days); intensity may vary<2 times a month Lung Function : FEV1 or PEF >80% predicted PEF variability <20% Mild Persistent Symptoms >2 times a week but <1 time a dayExacerbations may affect activity>2 times a month Lung Function: FEV1 or PEF >80% predicted PEF variability 20-30%
Asthma Severity staging of disease • Moderate Persistent : Daily symptomsDaily use of inhaled or short-acting b2-agonistExacerbations affect activityExacerbations >2 times a week; may last days • Night Time symptoms: >1 time a week • Lung Functions: FEV1 or PEF >60% - <80% predicted PEF variability >30% • Severe Persistent: Continued symptoms Limited physical activity Frequent exacerbations • Night Time symptoms: Frequent • Lung Functions: FEV1 or PEF <60% predicted PEF variability >30%
Asthma action plan: Adult self-management instructions. Important Peak Flow Numbers Baseline_________ L/min_______% Baseline=__________________L/min If your peak flow drops below ___________or you notice:—Increased use of inhaled treatments to manage asthma—Increased asthma symptoms upon awakening or at night. Follow these treatment steps: Increase inhaled steroids Take Two puffs of _____________FOUR times a day. Begin/increase treatment with oral steroids Take ___ mg of prednisone at _______ AM and/ or _______ PM If your peak flow number drops below __________or if you continue to get worse after treatment according to the directions above, follow these treatment steps. Begin/increase treatment with oral steroids Take ______mg of prednisone at _______AM and/ or _______PM Contact your health-care provider. if: Your peak flow number drops below_______. Asthma symptoms worsen while you are taking oral steroids Inhaled bronchodilators treatments are not lasting four hours If you can not contact your health care provider go directly to the ED. If you have questions call __________________ Date _________________Physician signature ________________Patient/Family signature_____________
ASTHMA treatment • Albuterol MDI: 4-8 puffs q 20 min up to 4 h, then every 1-4 h Nebulized:2.5-5 mg every 20 min for 3 doses, then 2.5-5 mg every 1-4 h or 10-15 mg/h continuously Dilute to minimum volume of 4 mL and gas flow of 6-8 L/min • Ipratropium bromide MDI: 4-8 puffs as neededNebulised: 0.5 mg every 30 min for 3 doses then every 2-4 h as needed May mix in same nebulizer with albuterol • Subcutaneous bronchodilatorsEpinephrine0.3-0.5 mg every 20 min for 3 doses SQ No proven long-term advantage over aerosol • Terbutaline0.25 mg every 20 min for 3 doses SQ No proven advantage over aerosol; use in pregnant patients • Corticosteroids Prednisone 120-180 mg/d in 3-4 doses for 48 h, then 60-80 mg/d until PEF >70% of predicted No advantage for higher doses • Methyl-prednisolone 40 mg IV every 6 h No advantage of IV over oral therapy, if patient tolerates oral medications • Other medicationsAminophylline0.6 mg/kg//h continuous infusion (keep level 8-15 g/mL) Not recommended*MDI=metered-dose inhaler