Download
1 / 43
430 likes | 551 Views
Freston Symposium. Fecal Microbiota Therapy (FMT) in the Management of C. difficile Infection (CDI). Lawrence J. Brandt, MD Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College of Medicine. Conflicts of Interest.

E N D
Freston Symposium Fecal Microbiota Therapy (FMT) in the Management of C. difficile Infection (CDI) Lawrence J. Brandt, MDEmeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College of Medicine
Conflicts of Interest Cipac: Advisory Board
Incidence and Impact of C. difficile ~ 500,000 cases~ $5 billion in excess costs~ 30,000 deaths annually Campbell et al. Infect Control Hosp Epidemiol. 2009:30:523-33 Dubberke et al. Emerg Infect Dis. 2008;14:1031-8 Dubberke et al. Clin Infect Dis. 2008;46:497-504 Elixhauser et al. HCUP Statistical Brief #50. 2008
ACG Rx Guidelines for CDI, 2013 Mild-moderateMZ (500 mg potid) x 10 days ♦ Strong recommend, high qualevid SevereVanco (125 mg poqid) x 10 days ♦ Cond recommend, mod qualevidif NRVanco (500 mg poqid) plus MZ (500 mg IV tid) ♦ Strong recommend, mod qualevid ComplicatedVancopo (125-500 mg qid) and pr (500 mg in 500 mL qid) plus MZ (500 mg IV tid) if ileus, toxic colitis, distention♦ Strong recommend, low qualevidconsider surgRx if: BP (pressors); sepsis, MOF; MS change; WBC≥50 K, lactate ≥5; no improvement (5d) ♦ Strong recommend, mod qualevid Am J Gastroenterol, 2013
Fidaxomicin vs Vanco 200mg BID x 10 d 125mg QID x 10 d @28d Louie TJ et al. N Engl J Med 2011; 364:422-431
Fidaxomicin is superior to Vanco for 1st CDI recurrence 36% (22/62) recurrence 20% (13/66)recurrence Cornely, OA et al. CID 2012:55 (Suppl 2); 154-61
Rifaximin“chaser” for Recurrent CDI Rifaxamin Placebo Standard therapy x 10-14 days (MZ , 82%; Vanco,18%) followed by: Placebo or Rifaximin (400 mg tid x 20 days) Garey et al. J Antimicrob Chemother 2011
Antibody and Vaccine Rx Antibodies RDBPC study of fully human monoclonal antibodies against C. difficile toxins A and B ♦administered as a single infusion (10mg/kg) ♦200 patients, receiving abx for active CDI ♦primary outcome: recurrence w/in 84 days - antibodies: 7%, placebo: 25%- pts with BI/NAP1/027: 8% vs 32% - pts with prior recurrence: 7% vs 38% Vaccines Sanofi announced (Aug 2013) starting late-stage trials (15,000 people) testing C. difficile vaccine Lowy I et al. N Engl J Med 2010; 362:197-205
Non-toxigenicC. difficile (NTCD) Strain VP 20261* Phase II trial (ViroPharma, Inc) • CDI patients on oral vancomycin • Placebo (n=43) • or NTCD (n=125) - 104 x 7 days (n=41) - 107 x 7 days (n=43) - 107 x 14 days (n=41) 2% CDI recurrence rate in colonized pts P<0.0001 P<0.01
Recurrent C.difficile Infection 15-20% of patients relapse re-infection post-C. difficile IBS 2nd recurrence: 30-45%; 3rd recurrence:45-60% Rx failure before 2003 <10%; after 2003 ~20% Relapses can continue for years No universal Rx algorithm Rxrecommendations are not evidence-based
Recurrent C.difficile Infection Why Do We Get It? Impaired host-response Altered intestinal microbiome
Firmicutes~76% Bacteroidetes~16% Spor A, Koren O, Ley R. Nature Reviews Microbiology, 2011
Decreased Diversity of the Fecal Microbiome in Recurrent C.difficile Patients with recurrent C.difficile have decreased phylogenetic richness Bacteroidetes and Firmicutes are reduced in patients with recurrent C.difficilenot in patients with just one episode of C.difficile infection Chang JY, et al. J Infect Dis 2008:197;435-8
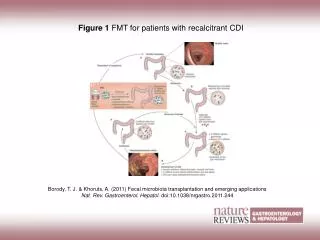
Mouse Model for C. difficile-Mediated Dysbiosis... and Successful FMT Homeostasis Antibiotic perturbation (clinda x 7d) Expansion of microbiota C. difficile(027/B1) Persistent dysbiosis Transient dysbiosis Disrupted dysbiosis↓shedding C. difficile Simplified microbiota↑pro-inflammatory genes↓ butyrate, acetate↑succinate Vanco BacterioRx (6 spp) or FMT or FMT Modified from: Lawley TD et al.. PLoS Pathog (2012); 8: e1002995.
ACG Rx Guidelines for CDI, 2013 Recurrent CDI1st: Can use same Rx as for initial episode; if severe, use Vanco 2nd: Pulsed vanco regimen ♦ Cond recommend, low qualevid 3rd: Pulsed-tapered Vanco; (no comparative data) - 125 mg daily pulsed Q3D for 10 doses -qidtid bid qdregimen -qid interval dosing (q2d, q3d, q4d) Consider FMT. ♦ Cond recommend, low qualevid Intravenous immune globulin (IVIG) may be helpful in hypo-gammaglobulinemic pts ♦ Strong recommend, low qualevid Am J Gastroenterol, 2013
Fecal Microbiota Transplantation (FMT) Definition: Instillation of stool from a healthy person into a sick person to cure a certain disease Rationale: A perturbed imbalance in our intestinal microbiota (dysbiosis) is associated with or causes disease and can be corrected by re-introduction of donor feces
Rationale for FMT in Recurrent CDI Avoid prolonged, repeated courses of antibiotics Re-establish normal diversity of the intestinal microbiome, thus restoring “colonization resistance”
Early History of FMT 4th century: Ge Hong described use of human fecal suspension by mouth for food poisoning or severe diarrhea “Zghou Hou Bei Ji Fang” (Handy Therapy for Emergencies) 16th century: Li Shizhen detailed prescriptions of fermented fecal solution, fresh fecal suspension, dry feces or infant feces for abdominal diseases with diarrhea, abdominal pain, fever, vomiting and constipation; “yellow dragon soup”“Ben Cao Gang Mu ” (Compendium of Materia Medica ) 17th century: veterinary medicine:transfaunation (transfer of cecal contents or fresh feces) from healthy horses to treat horses with chronic diarrhea rumen transfaunationis used to refaunate cows that have been off-feed because of mastitis or other illness
Later History of FMT 1958: Eismann et al. 4 pts with pseudomembranous colitis (Micrococcus pyogenes)Rxd with FMT enema 1983: Schwann, et al. CDI Rxd with FMT enema Other methods of FMT 1991: NG tube (Aas, Gessert, Bakken)1998: gastroscopy and colonoscopy (Lund-TØnnesen) 2000: colonoscopy (Persky, Brandt) 2010: self-administered enemas (Silverman, Davis, Pillai)
Protocol for FMT in Recurrent CDI Choose donor any healthy person universal donor Donor exclusions antibiotic use within 3 months diarrhea, constipation, IBS, IBD, colorectal CA, immunocompromise, anti-neoplastic drugs, high-risk behaviors: MSMP, recent body piercing or tattoo other: diabetes, obesity, atopy, ASCVD... ? psychologic or mood disorder, neurologic disease... Donor testing stool: culture (incl Listeria, Vibrios), O & P, C. difficile, H. pylori Ag, Giardia Ag, cryptosporidium, isospora, norovirus blood: hepatitis A, B, C, syphilis, HIV 1, 2 POOP
Protocol for FMT in Recurrent CDI Recipient D/C antibiotics 2-3 days before procedure? Large-volume colonoscopy prep the evening before procedure Loperamide before procedure? Donor Gentle laxative (e.g., MOM) the night before the procedure? Freshly passed stool is used within 6 hours Stool need not be refrigerated
Protocol for Colonoscopic FMT in Recurrent CDI Stool Transplant Donor stool → suspension with non-bacteriostatic saline mix by hand mix by blender Filtered through gauze into canister Use of a hood (stool is a level 2 biohazard) 60 cc catheter-tip syringe connected to “suction” tubing Volume of ~300cc instilled into ascending colon
Meta-analysis of Clinical Resolution Rates (11of 2709 reports, 273 patients) Resolution 90% overall lower: 91% upper: 82% No AEs Kassam et al . AM J Gastroenterol, 2013
FMT for Treatment of CDI: A Systematic Review Site of FMT # of Pts Dose of FMT(mean g/mls) Success Rate (%) Stomach 109 25/68 81 Duod/Jejunum 97 63/252 86 Cecum/Asc Colon 214 93/281 93 Distal Colon 116 58/272 84 Cammarota G, Ianiro G, Gasbarrini, A. J Clin Gastroenterol, 2014
Nasoduodenal FMT for Recurrent CDI: a RCT Study terminated by DSMB AEs: transient cramping, belchingSAEs: none van Nood E , Vrieze A , Nieuwdorp M et al. N Engl J Med 2013;368:407–15
Follow-up Survey 77 patients > 3 months after FMT Mean duration of illness: 11 monthsSymptomatic response after FMT mean of 6 days < 3 days in 74% Primary cure rate: 91 % Secondary cure rate: 98.7% 97% of patients would have another FMT for recurrent CDI and 58.3 % would choose FMT as their preferred Rx All late recurrences occurred in setting of subsequent unrelated antibiotics Brandt LJ, et al. Am J Gastroenterol, 2012
Cure Rates and AEsin 146 Patients > 65 years of Age Agrawal M, Aroniadis O, Brandt L, et al, DDW, 2014
HowDo Patients Feel About FMT? Hypothetical case scenarios given to clinic attendees (n=192) efficacy data alone (Floral Reconstitution) (85%) awareness of fecal nature of FR (81%) FMT chosen if by pill (90%) or if MD recommended (94%) FMT issues found most unappealing need to handle stool (65%) receiving FMT by NGT (75%) women: all aspects of FMT unappealing, “gross” (odor, handling stool) men: concerned with safety issues no signif diff in age or education level older patients: FMT less unappealing Zipursky, et al. Clin Infect Dis, 2013
HowDo Physicians Feel About FMT? 2010 (Kelly et al): 73 physicians 10% had performed FMT or knew a colleague who had 48% willing to try FMT 34% unwilling to try FMT 2013 (Sofi et al): 118 physicians (85GE, 32ID) 86% willing to do FMT 9% unwilling to do FMT need for published Guidelines concerns for safety Kelly, ACG meeting 2010; Sofi, Am J Gastroenterol 2013
FDA Regulations Early 2013. Fecal microbiota falls within the definition of a biologic product and a drug. Since FMT has not yet been approved by the FDA for any specific clinical indication, it constitutes an investigational agent and requires an Investigational New Drug application (IND) from Center for Biologics Evaluation and Research(CBER) . May, 2013. Public workshop on FMT July, 2013. FDA intends to exercise “enforcement discretion” regarding IND requirements for the use of FMT to treat C. difficile infection not responding to standard therapies…provided that the treating physician obtains [appropriate] adequate informed consent . Informed consent should include, at a minimum, a statement that the use of FMT products to treat C. difficile is investigational and a discussion of its potential risks.
FMT…the next steps A. Frozen fecal material from a universal donor* Donor MaterialNSuccess* Recurrence Pt-identified donor 10 7/10 (70%) 3/10 (30%) Std donor, fresh 12 11/12 (92%) Std donor, frozen 21 19/21 (90%) Total 43 37/43 (86%) 6/43 (14%) 3/33 (9%) 4 of 6 patients with RCDI had a 2nd FMT (std donor) all cleared their infection final success rate of 41/43 (95%) B. Synthetic stool (33 bacterial strains) from healthy donor (Repoopulate) # 2 patients cured of RCDI C. 3 strains of Bacteroides (ovatus, fragilis, thetaiotaomicron) 1 patient cured of RCDI D. Poop pills%: 27 patients took 24-34 pills all cured of RCDI # Petrov ,, et al. Microbiome 2013; Graham, ACG. 2013 *Hamilton, et al. Am J Gastroenterol 2012; %Thomas Louie, Univ of Calgary; ID week, 2013
Therapeutic unit of full-spectrum microbiota Petrof EO, Khoruts A. Gastroenterology 2014
Anatomy of a Robogut Petrof EO, Khoruts A. Gastroenterology 2014
LactateProducers SCFAProducers Methanogens MucinDegraders BioactiveMolecule Fecal Microbial Transplant Consortium Single strain Specificity Ecosystem Effects Modfied from Olle, B. Nature Biotechnology, 2013
Safety and Ethical Concerns Acute infectionsbacterial, viral, parasiticcolonic, systemic Acute allergic reactions Minor Long-term concernsis it possible that we are predisposing the recipient to (some, all) of the diseases /conditions that the donor will develop in his/her lifetime?have we created a microbiomic clone of the donor?forhow long will the donor microbiota populate the recipient’s colon?
Future Areas of Investigation IndicationsCDI:severe, complicated disease? 1st occurrence?other GI diseases: IBD, IBS, constipation non-GI diseases: diabetes, obesity, Parkinson’s, MS, autism? Route and means of administration Safety and ethical concerns: short-term: infections, allergies long-term: diseases of the donor, altered microbiota Product development processed stool → spec strains ± bioactive molecules
Solutions Use the safest product possiblestool is most problematicstool-derived product from volunteer population is probably safer bioengineered (commercial) product is safest Monitor results carefullynational registry for all FMT
Take Home Points Current guidelines are rational and initial routine care should be concordant with these recommendations Fidaxomicin is effective FMT has reached a “critical mass” and is likely the most appropriate salvage therapy currently available for multiply recurrent CDI. More robust (RCTs) data are needed. Concern for long-term sequelae FMT will be replaced by bioengineered product(s)