Download

1 / 19
200 likes | 368 Views
urine culture. Pathophysiology of urinary tract infection. Ascending route of infection is the most common. Hospital infection associated with lower urinary tract instrumentation (catheterization, cystoscopy).

E N D
Pathophysiology of urinary tract infection • Ascending route of infection is the most common. • Hospital infection associated with lower urinary tract instrumentation (catheterization, cystoscopy). • Once in the bladder uropathogens multiply, then pass up the ureters to the renal pelvis and parenchyma • Source of uropathogens: enteric bacteria mainly
Urinary tract infection more common in women than men • Short female urethra. • Close proximity to perianal areas. • Men also have an antibacterial substance in their prostate gland that reduces their risk.
Pathophysiology of urinary tract infection • Cystitis: (lower urinary tract infection) • Pyelonephritis: infection of the kidney • with acute suppurative inflammation of the • pelvis, • medullary and cortical tubules, • corticomedullary intersititum • Urosepsis: bacteremia due to pyelonephritis • Papillary necrosis • Sloughing of necrotic pyramids • Perinephric abscess
Risk factors in complicated urinary tract infection • Indwelling catheters • Urinary calculi • Neurogenic bladder • Prostatic enlargement • Uterine prolapse • Urologic instrumentation or surgery • Renal transplantation • Diabetes mellitus
Common uropathogens • Escherichia coli • Other Enterobacteriaceae (Klebsiella, Enterobacter, Proteus, Citrobacter) • Pseudomonas aeruginosa • Enterococcus • Staphylococcus saprophyticus • Staphylococcus aureus • Associated with staphylococcemia • Streptococcus agalactiae (group B) • Denotes vaginal colonization in pregnant women • Candida
Uncommon uropathogens • Corynebacterium urealyticum • Haemophilus influenzae and H. parainfluenzae • Blastomyces dermatitidis • Neisseria gonorrhaeae • Mycobacterium tuberculosis
Notes • Adult urine volume = 600 – 2500 ml /24hr. • Oligouria: marked decrease in urine flow < 400 ml/24hr. • Polyuria: Marked increase in urine flow > 2500 ml/24hr. • Anuria: less than 100 ml/24hr. • Nocturia: excessive urination during night.
Aim of the test • An etiological diagnosis of bacterial urinary tract infection by quantitative • Cultivation of the urine with identification and susceptibility test of the isolated bacteria(s). • Criteria of specimen rejection • Un-refrigerated specimen older than 2 hours may be subject to overgrowth • unlabeled specimen; mislabeled specimen; • Specimen in expired transport container
Types of urine specimens • First-voided morning urine optimal (generally bacteria have been proliferating in bladder urine for several hours) • Midstream urine specimens (initially voided urine contains urethral commensals) • Indwelling catheters (freshly placed, urine aspirated by needle inserted into catheter) (Foley catheter tips not acceptable) • Straight catheter specimens • Suprapubic aspirates (infants or children, recovery of anaerobes) • Cystoscopic collection of urine
Specimen collection • Male: • If not circumcised, draw back the foreskin. • Begin to urinate, but pass the first portion into the toilet. • Collect the mid-portion of urine into the container, and pass the excess into the toilet. • Female: • Squat over the toilet and separate the labia with one hand. • Void the first portion of urine into the toilet. • Collect the mid-portion of urine into the container and pass the excess into the toilet.
Collection of urine specimens • Urine collected in sterile specimen container must be processed within hours, or refrigerated and processed within 24 hours • Urine collected in sterile specimen container with borate preservative should be processed within 24 hours (no refrigeration required)
Catheterized urine • Cleanse periurethral area with soap and water • Insert catheter into bladder • Discard initial urine • Collect specimen in sterile cup • Chronic indwelling Foley catheter • Clamp tubing below junction (or port) • Disinfect with alcohol • Insert needle (on syringe) through port or catheter wall and aspirate. • DO NOT recontamination
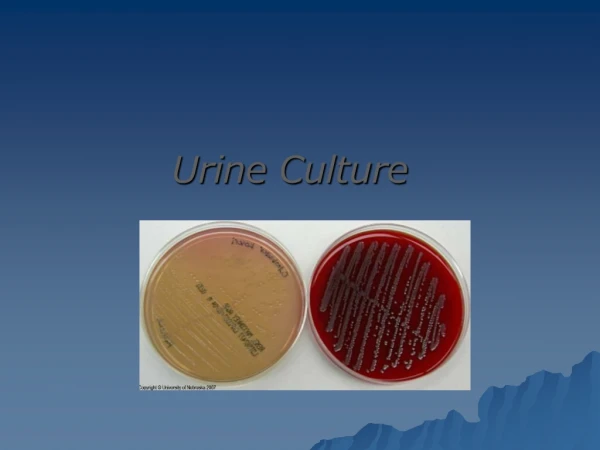
Inoculation of urine • Inoculation of urine for quantitative culture (colony forming units→ CFU’s) performed with a calibrated 0.001 mL(1µL) and 0.01 mL (10µL) plastic or wire loop • Nutrient agar or sheep blood agar utilized for quantitative urine culture • With 0.001 ml loop, 1 colony on SBA equivalent to 1,000 CFU’s per mL of urine • With 0.01 ml loop, 1 colony on SBA equivalent to 100 CFU’s per mL of urine • MacConkey agar utilized as selective differential agar for gram-negative bacteria
Interpretation: Clean Voided Specimen • Normal: <10,000 organisms per ml. • Organisms >10,000 per ml needs repeat urine culture? • Urinary Tract Infection • Boys • Organisms >10,000 per ml suggests UTI likely • Girls • Organisms >100,000 per ml suggests UTI • Three specimens: 95% probability of UTI • Two specimens: 90% probability of UTI • One specimen: 80% probability of UTI
Post specimen processing • Interfering factors: • Patient on antibiotic therapy. • Improper sample collection. • Result reporting: • Report wet mount as an initial report. • Report the isolated pathogen and its sensitivity pattern as a final report. • Turn around time: • Wet mount results should be available 1 hour after specimen receipt. • culture will be reported out 1-2 days after the receipt of the specimen. • Isolation of a possible pathogen can be expected after 2-3 days Negative