Download
1 / 46
550 likes | 1.31k Views
HYPERMETROPIA. The term hypermetropia is derived from hyper meaning “In excess” met meaning “measure” & opia meaning “of the eye”. Also called hyperopia / longsightedness First suggested in 1755 by KASTNER. DEFINITION

E N D
The term hypermetropia is derived from hyper meaning “In excess” met meaning “measure” & opia meaning “of the eye”. • Also called hyperopia / longsightedness • First suggested in 1755 by KASTNER
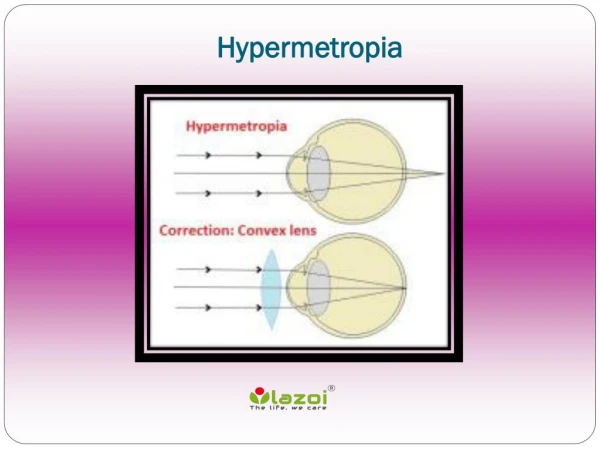
DEFINITION • It is the refractive state of eye where in parallel rays of light coming from infinity are focused behind the sentient layer of retina with accommodation being at rest • The posterior focal point is behind the retina which receives a blurred image
ETIOLOGY 1) AXIAL • Most common • Total refractive power of eye is normal • Axial shortening of eyeball • 1mm short- 3 D of HM • Physiologically more than 6D HM are uncommon • At birth +2.5 – 3 D of HM (physiologically) • Pathologically seen in cases like orbital tumour, inflammatory mass , oedema, coloboma and microphthalmos.
2) CURVATURAL • Flattening of cornea, lens or both • 1mm increase in Radius of curvature-RESULTS IN 6D of HM • Never exceed 6D HM physiologically • Congenitally flattened (cornea plana) • Result (trauma and disease ) 3) INDEX • Change in refractive index with age • Physiologically in old age • Pathologically in diabetics under treatment
4)POSITIONAL • Posteriorly placed crystalline lens • Occurs as congenital anomaly • Result of trauma or disease 5)ABSENCEOF LENS • Seen in aphakia
CLINICAL TYPES • SIMPLE HYPERMETROPIA, • PATHOLOGICAL • FUNCTIONAL HYPEROPIA
SIMPLE HYPERMETROPIA • Commonest form • Results from normal biological variations in the development of eyeball • Include axial and curvatural HM • May be hereditary
PATHOLOGICAL HYPERMETROPIA • Anomalies lie outside the limits of biological variation • Acquired hypermetropia • Decrease curvature of outer lens fibers in old age • Cortical sclerosis • Positional hypermetropia • Aphakia • Consecutive hypermetropia
FUNCTIONAL HYPERMETROPIA • Results from paralysis of accommodation • Seen in patients with 3rd nerve paralysis & internal ophthalmoplegia
OPTICAL CONDITION • Parallel rays focus behind retina • Diffusion circles produce blurred & indistinct images • Retina is nearer to nodal point • Image is smaller than in emmetropic • Rays diverge from retina • Formation of clear image is possible only when converging power of eye is increased
NOMENCLATURE TOTAL HYPERMETROPIA= LATENT + MANIFEST (facultative + absolute)
TOTAL HYPERMETROPIA • It is the total amount of refractive error,estimated after complete cycloplegia with atropine • Divided into latent & manifest
LATENT HYPERMETROPIA • Corrected by inherent tone of ciliary muscle • Usually about 1D • High in children • Decreases with age • Revealed after abolishing tone of ciliary muscle with atropine
MANIFEST HYPERMETROPIA • Remaining part of total hypermetropia • Correct by accommodation and convex lens • Measure by add strongest lens with max. vision • Consists of facultative & absolute FACULTATIVE HYPERMETROPIA • Corrected by patients accommodative effort ABSOLUTE HYPERMETROPIA • Residual part not corrected by patients accommodative effort Absolute hypermetropia can be measured by the weakest convex lens with which maximum visual acuity
MANIFEST HYPERMETROPIA CONT… • Manifest HM – absolute HM = Facultative HM (Strongest lens) – (weakest lens) • Total HM – Manifest HM = Latent HM
NORMAL AGE VARIATION • At birth +2+3D HM • Slightly increase in one year of life, • Gradually diminished untill by the age 5-10 years • In old age after 50 year again tendency to HM • Ton of ciliary muscle decreases • Accommodative power decreases • Some amount of latent HM become manifest • More amount of facultative HM become absolute • Practically after 65 year all of it become absolute
SYMPTOMS • Principal symptom is blurring of vision for close work • Symptoms vary depending upon age of patient & degree of refractive error ASYMPTOMATIC • small error produces no symptoms • Corrected by accommodation of patient
ASTHENOPIA • Refractive error are fully corrected by accommodative effort • Thus vision is normal • Sustained accommodation produces symptoms • Asthenopia increases as day progresses • Increased after prolonged near work SYMPTOMS Tiredness Frontal or fronto temporal headache Watering Mild photophobia
DEFECTIVE VISION WITH ASTHENOPIA • Not corrected by accommodation • Defective vision for near more than distance • Asthenopia due to sustained accommodation • Refractive error more(>4D)
DEFECTIVE VISION ONLY • Refractive vision more than 4D • Adults usually do not accommodate • Marked defective vision for near and distance
SIGNS • VISUAL ACUITY : Defective • EYEBALL: small or normal in size • CORNEA : may be smaller than normal. There can be CORNEA PLANA • ANTERIOR CHAMBER : may be shallow • LENS: could be dislocated backwards • A Scan ultrasonography (biometry) reveal short axial length
FUNDUS: • DISC: Dark reddish color, irregular margins ,confused with Papillitis so termed as PSEUDO-PAPILLITIS • MACULA: Situated further from the disc than usual, large positive angle alpha, apparent divergent squint • BLOOD VESSELS: Show undue tortuosity & abnormal branchings • BACKGROUND: SHOT- SILK RETINA
COMPLICATION • Recurrent styes m blepharitis or chalazia • Accommodative convergent squint • Amblyopia • Anisometropic • Stravismic • Uncorrective bilateral high hypermetropia • Predisposition to develop primary narrow angle glaucomas Care should be taken while instilling mydriatics
TREATMENT BASIS FOR TREATMENT • No Treatment • Error is small • Asymptomatic • Visual acuity normal • No muscular imbalance
Young children(<6 or 7yrs) • Some degree of hypermetropia is physiological so no correction • Treatment required if error is high or strabismus is present • working in school small error may require correction • In children error tends normally to diminish with growth so refraction should be carried out every six month and if necessary the correction should be reduced, ortherwise a lens which is overcorrecting their error may induce an artificial myopia • No deduction of tonus allowance in strabismus
ADULTS • If symptoms of eye-strain are marked,we correct as much of the total hypermetropia as possible,trying as far as we can to relieve the accommodation • When there is spasm of accommodation we correct the whole of the error • Some patients with hypermetropia do not initially tolerate the full correction indicated by manifest refraction so we undercorrect them • Exophoria hyperopia should be under correct by 1 to 2D
Patients with absolute hypermetropia are more likely to accept nearly the full correction because they typically experience immediate improvement in visual acuity • In pathological hypermetropia the underlying cause rather than the hypermetropia is chief concern
MODE OF TREATMENT • SPECTACLES • CONTACT LENS • SURGICAL OPTICAL TREATMENT
SPECTACLES Basic principle Prescribe convex lenses(Plus lenses) so that rays are brought to focus on the retina Advantages • Comfortable • Easier method • Less expensive • Safe idea
CONTACT LENS ADVANTAGES Cosmetically good Increased field of view Less magnification Elimination of aberrations & prismatic effect
REFRACTIVE SURGERY • Refractive surgery is not as effective as in myopia TYPES: (1)HEXAGONAL KERATOTOMY(HK) • Low to moderate degrees of hypermetropia • Its risk /benefit ratio is not low enough to warrant its continued use
LASER THERMAL KERATOPLASTY(LTK) • Procedure done using laser energy to heat the cornea (contraction of collagen) and increase its curvature • Central heating of cornea results in central corneal flattening thereby resulting in hyperopic shift
PHOTOREFRACTIVE KERATECTOMY(PRK) • Direct laser ablation of corneal stroma after removal of corneal epithelium mechanically • Done using EXCIMER LASER
LASER IN SITU KERATOMILEUSIS(LASIK) • Anterior flap of cornea lifted with keratome and excimer laser is used to sculpt the stromal bed to change the refractive error of eye • It can correct up to 4D of hypermetropia and 8D of astigmatism
PHAKIC IOL AND CLEAR LENS EXTRACTION • Done by Phaco technique • Clear lens extraction with the implantation of an IOL-----Preferably foldable IOL or a Piggyback IOL is implanted
VISUAL HYGIENE • While reading or doing intensive near work take a break about every 30 min • When reading maintain proper distance that is the book should be at least as far from your eyes as your elbow when you make a fist and hold it against your nose • Sufficient Illumination • Place a limit spent watching television & watching videogames • Sit 5-6 feet away from the television
Appropriate optical correction almost always leads to clear and comfortable single binocular vision • Younger children who have significant hyperopia associated with amblyopia, strabismus,or anisometropia require treatment, starting as early as 3-6 months of age
CONCLUSION • Hyperopia is a common refractive disorder that has been overshadowed by myopia in public perception,vision research & the scientific literature • Although uncorrected myopia has a greater adverse effect on visual acuity than uncorrected hyperopia,the close association between hyperopia,amblyopia & strabismus,especially in children,makes hyperopia a greater risk factor for more permanent vision loss than myopia
The early diagnosis & treatment of significant hyperopia & its consequences can prevent a significant amount of visual disability in the general population
THANK YOU For Further Queries Contact : Ms. Priyanka Singh Head – Optometry Service Email – optometry@venueyeinstitute.org