Download
1 / 1
20 likes | 194 Views
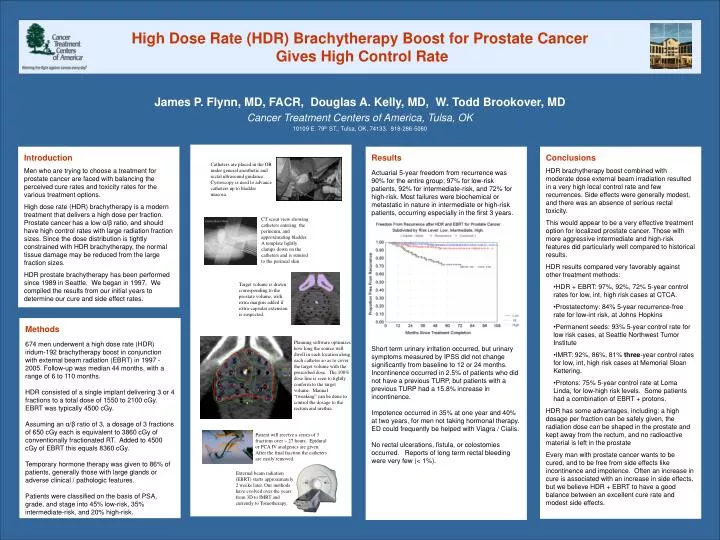
High Dose Rate (HDR) Brachytherapy Boost for Prostate Cancer Gives High Control Rate. James P. Flynn, MD, FACR, Douglas A. Kelly, MD, W. Todd Brookover, MD Cancer Treatment Centers of America, Tulsa, OK 10109 E. 79 th ST., Tulsa, OK, 74133. 918-286-5060. Results

E N D
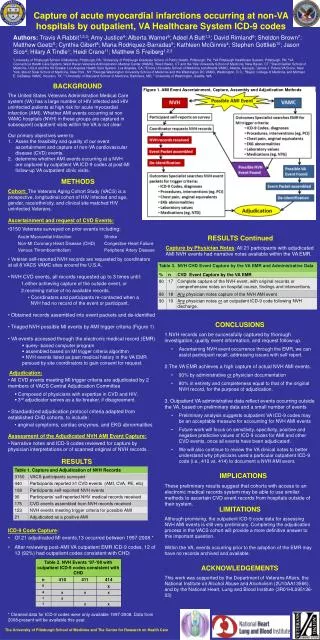
High Dose Rate (HDR) Brachytherapy Boost for Prostate Cancer Gives High Control Rate James P. Flynn, MD, FACR, Douglas A. Kelly, MD, W. Todd Brookover, MD Cancer Treatment Centers of America, Tulsa, OK 10109 E. 79th ST., Tulsa, OK, 74133. 918-286-5060 Results Actuarial 5-year freedom from recurrence was 90% for the entire group; 97% for low-risk patients, 92% for intermediate-risk, and 72% for high-risk. Most failures were biochemical or metastatic in nature in intermediate or high-risk patients, occurring especially in the first 3 years. Short term urinary irritation occurred, but urinary symptoms measured by IPSS did not change significantly from baseline to 12 or 24 months. Incontinence occurred in 2.5% of patients who did not have a previous TURP, but patients with a previous TURP had a 15.8% increase in incontinence. Impotence occurred in 35% at one year and 40% at two years, for men not taking hormonal therapy. ED could frequently be helped with Viagra / Cialis. No rectal ulcerations, fistula, or colostomies occurred. Reports of long term rectal bleeding were very few (< 1%). • Conclusions • HDR brachytherapy boost combined with moderate dose external beam irradiation resulted in a very high local control rate and few recurrences. Side effects were generally modest, and there was an absence of serious rectal toxicity. • This would appear to be a very effective treatment option for localized prostate cancer. Those with more aggressive intermediate and high-risk features did particularly well compared to historical results. • HDR results compared very favorably against other treatment methods: • HDR + EBRT: 97%, 92%, 72% 5-year control rates for low, int, high risk cases at CTCA. • Prostatectomy: 84% 5-year recurrence-free rate for low-int risk, at Johns Hopkins • Permanent seeds: 93% 5-year control rate for low risk cases, at Seattle Northwest Tumor Institute • IMRT: 92%, 86%, 81% three-year control rates for low, int, high risk cases at Memorial Sloan Kettering. • Protons: 75% 5-year control rate at Loma Linda, for low-high risk levels. Some patients had a combination of EBRT + protons. • HDR has some advantages, including: a high dosage per fraction can be safely given, the radiation dose can be shaped in the prostate and kept away from the rectum, and no radioactive material is left in the prostate • Every man with prostate cancer wants to be cured, and to be free from side effects like incontinence and impotence. Often an increase in cure is associated with an increase in side effects, but we believe HDR + EBRT to have a good balance between an excellent cure rate and modest side effects. Introduction Men who are trying to choose a treatment for prostate cancer are faced with balancing the perceived cure rates and toxicity rates for the various treatment options. High dose rate (HDR) brachytherapy is a modern treatment that delivers a high dose per fraction. Prostate cancer has a low α/β ratio, and should have high control rates with large radiation fraction sizes. Since the dose distribution is tightly constrained with HDR brachytherapy, the normal tissue damage may be reduced from the large fraction sizes. HDR prostate brachytherapy has been performed since 1989 in Seattle. We began in 1997. We compiled the results from our initial years to determine our cure and side effect rates. Catheters are placed in the OR under general anesthetic and rectal ultrasound guidance. Cystoscopy is used to advance catheters up to bladder mucosa. CT scout view showing catheters entering the perineum, and approximating bladder. A template lightly clamps down on the catheters and is sutured to the perineal skin. Target volume is drawn corresponding to the prostate volume, with extra margins added if extra-capsular extension is suspected. Methods 674 men underwent a high dose rate (HDR) iridum-192 brachytherapy boost in conjunction with external beam radiation (EBRT) in 1997 - 2005. Follow-up was median 44 months, with a range of 6 to 110 months. HDR consisted of a single implant delivering 3 or 4 fractions to a total dose of 1550 to 2100 cGy. EBRT was typically 4500 cGy. Assuming an α/β ratio of 3, a dosage of 3 fractions of 650 cGy each is equivalent to 3860 cGy of conventionally fractionated RT. Added to 4500 cGy of EBRT this equals 8360 cGy. Temporary hormone therapy was given to 86% of patients, generally those with large glands or adverse clinical / pathologic features. Patients were classified on the basis of PSA, grade, and stage into 45% low-risk, 35% intermediate-risk, and 20% high-risk. Planning software optimizes how long the source will dwell in each location along each catheter so as to cover the target volume with the prescribed dose. The 100% dose line is seen to tightly conform to the target volume. Manual “tweaking” can be done to control the dosage to the rectum and urethra. Patient will receive a series of 3 fractions over ~ 27 hours. Epidural or PCA IV analgesics are given. After the final fraction the catheters are easily removed. External beam radiation (EBRT) starts approximately 2 weeks later. Our methods have evolved over the years from 3D to IMRT and currently to Tomotherapy.