Download
1 / 30
• 310 likes • 338 Views
Learn the fundamentals of CT imaging, identify basic cerebral anatomy, and develop an approach to CT interpretation. Explore the uses, pros, and cons of CT scans and understand how to identify pathologic lesions. Discover the basics of CT density and key brain structures. Improve your ability to read and interpret CT scans effectively with detailed insights and practical tips.

E N D
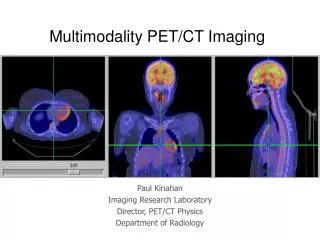
Introduction to CT and CTA Imaging Principles Ryan Hakimi, DO, MS Associate Professor Director, Critical Care Neurology Emmaculate Fields, APRN-CNP Clinical Instructor Department of Neurology The University of Oklahoma Health Sciences Center
DISCLOSURES • FINANCIAL DISCLOSURE • Nothing to disclose • UNLABELED/UNAPPROVED USES DISCLOSURE • Nothing to disclose • Some of the slides have been adapted from teaching materials used at the University of Oklahoma Health Sciences Center
LEARNING OBJECTIVES Upon completion of this course, participants will be able to: • Understand the basics of CT imaging • Identify and describe basic cerebral anatomy • Establish an approach to CT interpretation (ABBBC) • Identify pathologic lesions found on cranial CT
CT BASICS • CT uses x-rays • Provides axial brain view • CT scan is a density based study- measures density of the tissue being studied • Pros: fast, quickly accessible, cost-effective, less claustrophobia limitations, good for bone/fracture & fresh hemorrhage imaging • Cons: radiation exposure, fair tissue imaging cannot detect blood flow, iodinated contrast, brainstem, poor posterior fossa imaging (artifact)
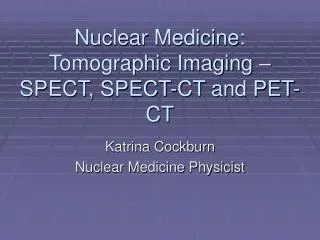
CT Brain axial view • CT uses x-rays to make cross-sectional axial images • Right is on left and vice-versa. Patient lying on a stretcher with feet coming toward you and is slid through a large open ring (CT machine) • Lateral view of skull is shown with imaging planes indicated by lines. The true horizontal plane is approximated by the orbitomeatal line, while the typical CT imaging plane is angled slightly upward anteriorly
SLICE A SLICE B SLICE C C B A CT Brain: Cranial Fossae POSTERIOR CRANIAL FOSSA (CEREBELLUM) MIDDLE CRANIAL FOSSA (TEMPORAL LOBE) ANTERIOR CRANIAL FOSSA (FRONTAL LOBE) Progressing from inferior to superior, axial slices first visualize posterior fossa, then middle fossa, then anterior fossa of skull
CT BASICS-density • Black White
ocular lenses bone contrast (dye) calcifications acute blood metal (bullets w/ streak artifact) Hyperdense things on CT- Bone, calcium, acute hemorrhage & contrast
Isodense things on CT-Brain parenchyma • Brain parenchyma is light gray • White matter is darker than gray matter Gray matter (cerebral cortex) Gray matter (basal ganglia) White matter
fat air CSF = water Hypodense things on Ct scan - CSF is very dark, sulci, cisterns & ventricles - Air , nasal cavity, sinuses, mastoid air cells
Normal Brain anatomy Nose Eye Sphenoid bone Temporal lobe Clivus Petrous bone Mastoid air cells Pons Cerebellum
Normal Brain anatomy Eye Sella turcica Optic nerve Petrous bone Mastoid air cells Sphenoid bone Temporal lobe Pons 4th ventricle Cerebellum
Normal Brain anatomy Interhemispheric fissure Frontal lobe Sylvian fissure Third ventricle Temporal lobe Sylvian aqueduct Cerebellum (vermis) Occipital lobe Falx
Normal Brain Anatomy Frontal lobe Interhemispheric fissure Corpus callosum (genu) Caudate nucleus (body) Lateral ventricle (body) Corona radiata (white matter) Parietal lobe Falx
Normal Brain Anatomy Frontal lobe Interhemispheric fissure and falx Centrum semiovale (white matter) Parietal lobe
CT BASICS-Windowing • Windowing allows the CT reader to evaluate the CT with subtle differences in tissue densities. • Acute ischemic window W30 L36: gray and white matter differentiation • Blood window W88 L40: acute hemorrhage • Brain window W130 L50: evaluation of soft tissue, CSF spaces. • Bone window W2000 L300: detailed evaluation for fractures • Default window or mostly used W30 L36
Approach to reading a CT scan- ABBBC • A- Air-filled structures (nasal cavity, sinuses, mastoid air cells) • B- Bones (fractures) • B- Blood (subarachnoid, intracerebral, subdural, epidural hematoma) • B- Brain tissue (infarction, edema, masses, brain shift • C- CSF spaces (sulci, ventricles, cisterns, hydrocephalus, atrophy)
A- Air-filled Structures • Normal air spaces are black both on bone and brain window. • Frontal, maxillary, ethmoid, and sphenoid are air-filled with no thickening of the mucosa or air fluid level. • Mastoids are spongy bone filled with tiny pockets of air. When these pockets are opacified you will see a (gray or white) shade. • Air-fluid levels in the setting of trauma suspect a fracture • Mastoid opacification without trauma indicates mastoiditis.
B- Bones • Useful when trauma is suspected • Window your image for bone reading • Recognize normal suture structures (usually available on both sides) • If fracture suspected, inspect the opposite side for similar finding. If not present then look for abnormalities associated with the fracture (air/pneuomocephalus, black spots with the hemorrhage)
B- Blood • Use windowing +60 to 80, determine the Location and shape of the blood • Epidural hematoma: over brain convexity, not crossing suture line, lens shaped (biconvex). • Subdural hematoma: over brain convexity, interhemispheric, along the tentorium, SDH will cross suture lines & it’s crescent shaped. • Intraparenchymal/Intracerebral hemorrhage: within the brain matter, sizes/shape varies dependent on etiology can be regular or irregular. • Interventricular hemorrhage- inside ventricles, can be isolated and or secondary to SAH, ICH. • Subarachnoid hemorrhage- blood within the subarachnoid spaces (sulci, sylvian fissure, cisterns). Usually assumes shape of the surrounding cerebral structure. • Density/age of blood • Hyperdense: Acute hemorrhage which is bright white usually < 4 days old • Isodense: Sub acute Hemorrhage will be same density as the brain usually 4 days to 2 weeks old • Hypodense: Old hemorrhage will be darker than brain tissue usually > 2-3 weeks
B- Brain tissue: Infarction, edema, masses, brain shift • Evaluate brain for symmetry, neoplasms, infarction and edema. • Neoplasms: though hard to visualize on a non contrast CT, mostly hypodense but can be hyperdense or isodense depending on type and stage, usually with edema surrounding the lesion. • Infarction: Hypodense, usually not able to be visualized on CT for the first 6 to 12 hours and is usually in a vascular distribution. Look for a hyperdense MCA sign, HU > 45 to avoid false positives. • Edema: evaluate if associated with a lesion, sulcal effacement. Loss of gray white differentiation, vasogenic edema usually does not follow vascular territories.
C-CSF structures • C- CSF spaces (sulci, ventricles, cisterns, hydrocephalus, atrophy) • Is there any sulcal effacement? • Are all the cisterns present? • Any blood in the cisterns? • Evaluate size of ventricles, any blood in the ventricles ?
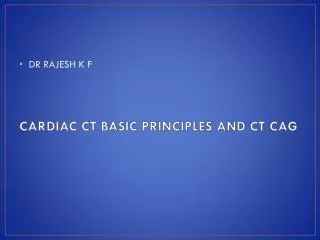
BRAIN CTA principles • Contrast is used to further evaluate cerebral vasculature (aneurysms, injury-dissection, vascular malformations, blockages- atherosclerosis) • Use of iodinated contrast injected rapidly through a vein and images are obtained as the contrast bolus travels through the intracranial vessels
CTA • X-ray based study with injection of dye to look at vessels • Advantages • Rapid, easily available for detecting intracranial occlusions and vessel visualization. • Less invasive vs catheter based angiogram • Coagulopathy not a major factor as no need for arterial access
CTA • Disadvantages • Radiation • Risk for contrast induced nephropathy (presence of renal insufficiency, diabetes or prediabetes) • Contraindications • Pregnant women (may shield if absolutely needed) • Iodine contrast allergies
References • Blumenfeld, H. (2010). Neuroanatomy through clinical cases (2nd ed.). Sunderland, Mass.: Sinauer Associates. • Perron, A(2005). Blood Can Be Very Bad: CT interpretation for the EM Physician. Foundation for Education and Research in Neurological Emergencies. Retrieved December 16, 2015 from http://www.uic.edu/com/ferne/pdf/acep_200 5_peds/perron_ich_acep_2005_peds...