Download
1 / 1
10 likes | 183 Views
Delayed Onset Endophthalmitis Rohit Adyanthaya, M.D. Department of Medicine, Good Samaritan Hospital, Baltimore, MD.

E N D
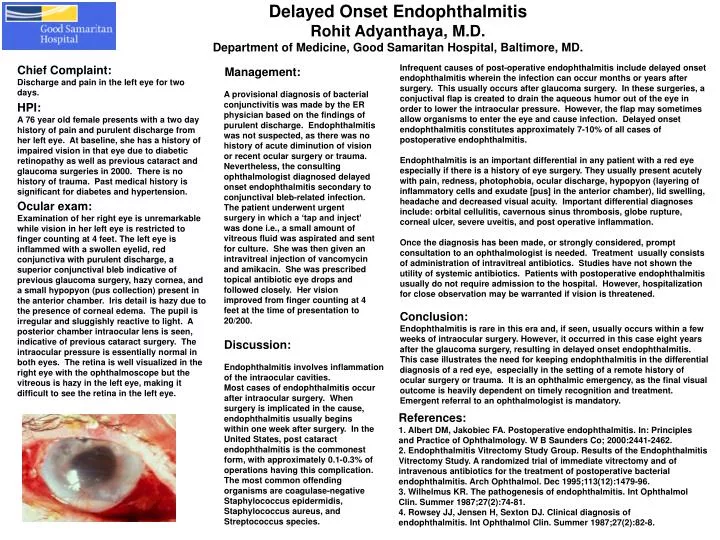
Delayed Onset Endophthalmitis Rohit Adyanthaya, M.D. Department of Medicine, Good Samaritan Hospital, Baltimore, MD. Infrequent causes of post-operative endophthalmitis include delayed onset endophthalmitis wherein the infection can occur months or years after surgery. This usually occurs after glaucoma surgery. In these surgeries, a conjuctival flap is created to drain the aqueous humor out of the eye in order to lower the intraocular pressure. However, the flap may sometimes allow organisms to enter the eye and cause infection. Delayed onset endophthalmitis constitutes approximately 7-10% of all cases of postoperative endophthalmitis. Endophthalmitis is an important differential in any patient with a red eye especially if there is a history of eye surgery. They usually present acutely with pain, redness, photophobia, ocular discharge, hypopyon (layering of inflammatory cells and exudate [pus] in the anterior chamber), lid swelling, headache and decreased visual acuity.Important differential diagnoses include: orbital cellulitis, cavernous sinus thrombosis, globe rupture, corneal ulcer, severe uveitis, and post operative inflammation. Once the diagnosis has been made, or strongly considered, prompt consultation to an ophthalmologist is needed. Treatment usually consists of administration of intravitreal antibiotics. Studies have not shown the utility of systemic antibiotics. Patients with postoperative endophthalmitis usually do not require admission to the hospital. However, hospitalization for close observation may be warranted if vision is threatened. Conclusion: Endophthalmitis is rare in this era and, if seen, usually occurs within a few weeks of intraocular surgery. However, it occurred in this case eight years after the glaucoma surgery, resulting in delayed onset endophthalmitis. This case illustrates the need for keeping endophthalmitis in the differential diagnosis of a red eye, especially in the setting of a remote history of ocular surgery or trauma. It is an ophthalmic emergency, as the final visual outcome is heavily dependent on timelyrecognition and treatment. Emergent referral to an ophthalmologist is mandatory. Management: A provisional diagnosis of bacterial conjunctivitis was made by the ER physician based on the findings of purulent discharge. Endophthalmitis was not suspected, as there was no history of acute diminution of vision or recent ocular surgery or trauma. Nevertheless, the consulting ophthalmologist diagnosed delayed onset endophthalmitis secondary to conjunctival bleb-related infection. The patient underwent urgent surgery in which a ‘tap and inject’ was done i.e., a small amount of vitreous fluid was aspirated and sent for culture. She was then given an intravitreal injection of vancomycin and amikacin. She was prescribed topical antibiotic eye drops and followed closely. Her vision improved from finger counting at 4 feet at the time of presentation to 20/200. Chief Complaint: Discharge and pain in the left eye for two days. HPI: A 76 year old female presents with a two day history of pain and purulent discharge from her left eye. At baseline, she has a history of impaired vision in that eye due to diabetic retinopathy as well as previous cataract and glaucoma surgeries in 2000. There is no history of trauma. Past medical history is significant for diabetes and hypertension. Ocular exam: Examination of her right eye is unremarkable while vision in her left eye is restricted to finger counting at 4 feet. The left eye is inflammed with a swollen eyelid, red conjunctiva with purulent discharge, a superior conjunctival bleb indicative of previous glaucoma surgery, hazy cornea, and a small hypopyon (pus collection) present in the anterior chamber. Iris detail is hazy due to the presence of corneal edema. The pupil is irregular and sluggishly reactive to light. A posterior chamber intraocular lens is seen, indicative of previous cataract surgery. The intraocular pressure is essentially normal in both eyes. The retina is well visualized in the right eye with the ophthalmoscope but the vitreous is hazy in the left eye, making it difficult to see the retina in the left eye. Discussion: Endophthalmitis involves inflammation of the intraocular cavities. Most cases of endophthalmitis occur after intraocular surgery. When surgery is implicated in the cause, endophthalmitis usually begins within one week after surgery. In the United States, post cataract endophthalmitis is the commonest form, with approximately 0.1-0.3% of operations having this complication. The most common offending organisms are coagulase-negative Staphylococcus epidermidis, Staphylococcus aureus, and Streptococcus species. References: 1. Albert DM, Jakobiec FA. Postoperative endophthalmitis. In: Principles and Practice of Ophthalmology. W B Saunders Co; 2000:2441-2462. 2. Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. Dec 1995;113(12):1479-96. 3. Wilhelmus KR. The pathogenesis of endophthalmitis. Int Ophthalmol Clin. Summer 1987;27(2):74-81. 4. Rowsey JJ, Jensen H, Sexton DJ. Clinical diagnosis of endophthalmitis. Int Ophthalmol Clin. Summer 1987;27(2):82-8.