Download
1 / 13
130 likes | 350 Views
Surgery for Ewing’s Sarcoma of Bone: Should We Excise the Pre or Post Chemotherapy Tumour Volume?. T.B.Beckingsale , S.A.Murray , P.Dildey , C.H.Gerrand , and the North of England Bone and Soft Tissue Tumour Service, Newcastle upon Tyne, UK.

E N D
Surgery for Ewing’s Sarcoma of Bone: Should We Excise the Pre or Post Chemotherapy Tumour Volume? T.B.Beckingsale, S.A.Murray, P.Dildey, C.H.Gerrand, and the North of England Bone and Soft Tissue Tumour Service, Newcastle upon Tyne, UK. T.B.Beckingsale, A.Griffin, J.Wunder, P.Ferguson, and the Musculoskeletal Oncology Team at Mt Sinai Hospital, Toronto, Canada.
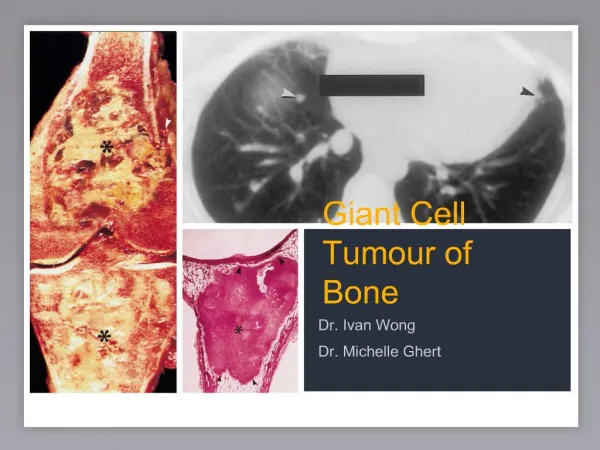
Introduction • James Ewing 1866 -1943 • Malignant small, round, blue cell tumour. • Treatment usually entails chemotherapy and surgery +/- radiotherapy. • Decisions and dilemmas regarding surgery.
The Problem Pre-Chemotx Post-Chemotx
The Problem Post-Chemotx Pre-Chemotx
What Should We Resect? • Does oedema = tumour? (1) • Cannot predict necrosis with imaging. (2) • 100% necrosis vs clonal resistance. 1. White et al. Histologic Assessment of Peri-Tumoral Edema in Soft Tissue Sarcoma. Int J Radiat Oncol Biol Phys. 2005 Apr 1;61(5):1439-45. 2. Denecke et al. Assessment of Histological Response of Paediatric Bone SarcomasUsing FDG PET in Comparison to Morphological Volume Measurement and Standardized MRI Parameters. Eur J Nucl Med Mol Imaging. 2010 Oct;37(10):1842-53.
Methods • Pre and Post chemotx tumour volumes on MRI compared to the volumes of resection specimens and their recorded margins. • Tumour volume NOT extent of oedema. • MRI volumes as per EURO-EWING protocol. • Cylindrical = A x B x C x 0.75 • Spherical = A x B x C x 0.52
The Study • Database patients: 57 (UK) & 46 (Canada) • Exclusions: • Retroperitoneal, head and neck, axial tumours. • Inappropriate surgery elsewhere. • Incomplete data. • UK: 8 patients. 3 M, 5 F. Av age 22 (6-52). • Canada: 13 patients. 7 M, 6 F. Av age 25 (18-53).
Results • MRIs • Tumour volume reduced in all cases with chemotherapy. • Pathology • Resection specimen volumes exceeded the pre chemotherapy tumour volumes in all cases in both centres. • Longitudinal dimension of resection specimen the primary reason for this.
Results: Freeman Hospital, UK • AP and ML resection specimen dimensions more closely match the post-chemotx tumour volume. • 4 patients: 100% necrosis • 2 patients: microscopically positive margin. (Both poor response to chemotx) • 2 patients close but clear margin: 1mm. • All pts received radiotx. • No LR. • 3 metastatic. • F/U Average 42 months (12-81)
Results: Mt Sinai Hospital, Canada • AP and ML dimensions more closely match the pre-chemotx tumour volume. • 3 patients: 100% necrosis • 1 patients: microscopically positive margin. • 1 patients close but clear margin: 1mm. • 8 patients: Wider margin. • No pts received radiotx. • No LR. • 1 metastatic. • F/U Average 23.5 months (1-82)
Conclusions • Hypothesis generating only but it seems that… Resection specimens that more closely match the post-chemotx tumour volume are more likely to result in microscopically positive or close margins if chemotx response is incomplete.
Conclusions • Unable to draw conclusions on LR and OS given power of study. • ? Risk of radiotx. (1) • ? Which approach is best. • ? Opportunity for further study. • National Ewing’s MDT in England. Ginsberg et al.Long-term Survivors of Childhood Ewing Sarcoma: Report From the Childhood Cancer Survivor Study. JNCI. 2010;102(16):1272-1283.