Download

1 / 10
100 likes | 122 Views
Learn how NHS Sunderland CCG aims to achieve better outcomes for Sunderland's population through improved out-of-hospital care services.

E N D
BETTER HEALTH AND CARE FOR SUNDERLAND Ian Holliday Head of Reform and Joint Commissioning NHS Sunderland Clinical Commissioning Group (CCG)
AIM: BETTER HEALTH AND CARE FOR SUNDERLAND Key Objective: To transform out of hospital care to achieve better outcomes for people and the whole system.
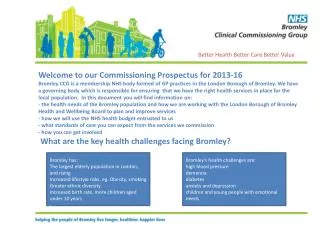
SUNDERLAND THE PLACE • 283,000 people in Sunderland • A population increase of 8,100 (3%) forecast over next 20 years • 37% increase amongst those aged 65-84 • 105% increase amongst those aged 85+ • Life expectancy in Sunderland is 78 for males and 82 for females (approx. 2% lower than the England average) Supply Characteristics: • CCG Co terminus with the LA • 1 main acute trust • 1 community services provider ( provided by neighbouring acute trust across 3 CCGs) • Large MH trust covering 13 CCGs • 51 Member Practices organised in 5 Localities • 660m budget for health and social care; 180 on acute of which 55 m non elective; 152m in BCF re OOH care • Organisations whose focus is Sunderland need to save over 15Om by 18/19 Map showing population density of Sunderland Population characteristics Sunderland North Washington Galleries Health Centre Sunderland West Sunderland East Coalfield High Low Population Density Source: ONS Statistics, Sunderland CCG Prospectus and Business Plan
The population cost pyramid indicates that the top 3% of patients drive 50% of cost in Sunderland Population cost segmentation, secondary care, community and mental health spend, 20131 Population segments Cost breakdown Spend per head: High Cost Over £5,000 per year 3 % 9 .7k 50%£106m £10.9k 12% 34k Moderate Cost £1,000 to £5,000 per year 36%£77m £2.2k 84% 239k2 Low Cost Under £1,000 per year 14% £29m £0.1k Source: Sunderland CCG secondary, community care and mental health data, Oliver Wyman analysis 1 – 2013 for secondary care and MH, March 2013 to Feb 2014 for community care 2 – 127k registered patients with no secondary, community or mental health interactions
Average Frail Elder without Cancer or Specialist Dementia care(2,000 patients in segment – 73% of Frail Elders)Frail Elders have diverse needs and use all care settings heavily Service utilisation • Reasons for admission (Top Primary Diagnosis CCS Codes) • 87 – Retinal detachments; defects; vascular occlusion; and retinopathy (7%) • 122 – Pneumonia (except that caused by tuberculosis or sexually transmitted disease) (6%) • 127 – Chronic obstructive pulmonary disease and bronchiectasis (5%) • 159 – Urinary tract infections (5%) • 108 – Congestive heart failure; nonhypertensive (3%) Source: Sunderland CCG secondary, community care and mental health data, Oliver Wyman analysis 1 – 2013 for secondary care and MH, March 2013 to Feb 2014 for community care 2 – Estimates based upon previous work
WHAT NEEDS TO BE DIFFERENT? CASE FOR CHANGE – Accelerated Solutions Event George now George’s improved journey George is 78 years old and has lived within Hendon Care Home for the last two years. Prior to moving to the Care Home, George lived alone in Southwick following the death of his wife. George has two children: a daughter, Julie, who lives in Houghton with her two children and a son who moved to Nottingham with his work. Three years ago, George suffered his first stroke and following treatment on the acute stroke ward at Sunderland Royal Hospital and support to return home from the Community Stroke Rehabilitation Team, George managed to continue to live in his own home for a further 9 months, with support from Home Care staff. During the 9 months, George became frightened to go out alone, which meant he didn’t meet up with his friends as often as he did. George is an avid Sunderland Football supporter and was a season ticket holder until he had his stroke. If George wasn’t watching football, he also enjoyed playing bowls for his local bowls club; this was George’s way of keeping himself ‘fit and active’. Unfortunately, George experienced a second stroke, which left him with significant disabilities. George is unable to move parts of his body, suffers from double incontinence, has difficulty in swallowing and often chokes and becomes agitated quite quickly due to the effects of his stroke. Despite the best efforts of everyone concerned with George’s care and treatment, George moved into Hendon Nursing Care Home. In the care home George was assessed by the link nurse who also arranged for the community geriatrician to see him. Some of his medications were changed and they have involved Physiotherapyto see if his mobility can be increased. The Dieticianhas also been consulted as George has been losing weight despite eating relatively well. George has had a number of UTIs, resulting in admissions to hospital for treatment. He is expressing anxiety about having to go into hospital and just wants to stay at home. George has been well cared for within the Care Home; with his daughter and grandchildren visiting as often as possible. He has made new friends, however often gets frustrated with some of his fellow residents, especially those who have dementia symptoms; spending more and more time on his own in his room.
In Summary • The challenge in Sunderland, both financial and demographic, is significant • No change is not an option – we must do things differently • All stakeholders are now working together to deliver this ambitious agenda