Download
1 / 16
170 likes | 441 Views
Impact of Cascade Reporting of Antimicrobial Susceptibility on the Consumption of Fluoroquinolone Antibiotics at a Veterans Affairs Medical Center Stewardship Interest Group Antibiotic Stewardship Research Symposium. Nicole C. Vissichelli, MD, Jane A Cecil, MD, Chris Einspahr , MSc,

E N D
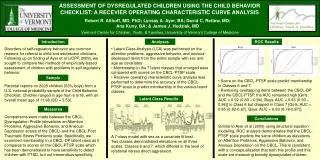
Impact of Cascade Reporting of Antimicrobial Susceptibility on the Consumption of Fluoroquinolone Antibiotics at a Veterans Affairs Medical CenterStewardship Interest Group Antibiotic Stewardship Research Symposium • Nicole C. Vissichelli, MD, • Jane A Cecil, MD, • Chris Einspahr, MSc, • Betty A Forbes, PhD, • Emily M. Hill, PhD, MT (ASCP), • Michael P. Stevens, MD, MPH, • Dan Tassone, PharmD, • Leroy B. Vaughan, MD • J. Daniel Markley, MD, MPH
Outline Introduction • Fluoroquinolone as a target for antibiotic stewardship programs • Role of Cascade and Selective Reporting Study Objectives Methods Results 5. Conclusions
Introduction: Fluoroquinolone Use Fluoroquinolone Use
Introduction • Fluoroquinolones (FQ) are one of the most common overprescribed antibiotics • 7.9 billion prescriptions in 2014 for conditions that did not require antibiotics or FQ were not first-line recommended agent • In a prospective observational study by Werner et al, 39% days of FQ therapy deemed unnecessary Werner et al BMC Infect Dis 2011. 11:187. Kabbanni et al. CID. 67(1) 2018: 134-146.
Introduction • Selective and cascade reporting (CSR) is a core strategy ASPs can utilize to nudge frontline providers to choose appropriate, narrow spectrum, antibiotics when possible • Limited data available regarding direct impact of CSR on prescribing • Evidence suggests CSR associated with decreased FQ prescribing Barlem et al. CID. 2016;62(10) e51-e77, Coupat et al Eur J Clin Microbiol Infect Dis. 2013;32(5):627-36, Tan et al J Antimicrob Chemother. 2013. Feb;51(2):379-84. Lanford et al. J Clin Microbiol. 2016. 54(9):2343-7
Study Objectives • To evaluate the impact of CSR on the consumption of FQs, amoxicillin/clavulanate (A/C), and trimethoprim/sulfamethoxazole (TMP-SMX) antibiotics
Methods Study type: Quasi-experimental Study duration: October 2017-September 2018 Setting: 399-bed tertiary care VAMC in Richmond, Virginia
Methods • Selective reporting algorithms were developed by genus of bacteria based on the following: • Local antibiogram • Practice guidelines for infectious diseases • Multidisciplinary team (ASP members, infectious disease physicians, microbiology laboratory leadership, executive leadership) • Several follow up meetings to troubleshoot and refine algorithms
Algorithm used for selective and cascade reporting for Enterobacteriaceae family *if ceftriaxone R, presume ESBL phenotype and report amoxicillin-clavulanate, ampicillin, cefazolin (if urine culture), ceftriaxone, cefepime, and piperacillin-tazobactam as “R” **Report only for urine isolates of E coli only Italics = do not report on CSF isolates
Methods • Aggregate facility-wide data was extracted from CDC’s NHSN AU module as antimicrobial days of therapy per 1000 days present for 6 months pre- and post-implementation of CSR • Analysis: • t test to determine difference in FQ consumption after CSR • Cohen’s d used to calculate effect size
Results • After initiation of CSR, mean ciprofloxacin use decreased by 29% with an effect size of -0.711 (p<0.05) • Mean levofloxacin use decreased by 10% with an effect size of -0.264 (p=0.422) • Mean use of A/C and TMP-SMX increased by 28% and 2% with an effect size of 0.577 and 0.043, respectively
Conclusions Implementing CSR was associated with a statistically significant reduction in mean ciprofloxacin use Levofloxacin use decreased after CSR implementation, although not significantly There was a corresponding increase in consumption of amoxicillin/clavulanate and trimethoprim/sulfamethoxazole CSR is a viable strategy that can be implemented by ASPs to reduce FQ consumption More data is needed to further trend antibiotic consumption over a longer time interval
Future Directions • Further investigation is needed to evaluate the impact of CSR on • appropriateness in reduction of FQ use • alternative antibiotic prescribing • resistance profiles • adverse drug events • Clostridioides difficile infection rates
Acknowledgements J. Daniel Markley, MD, MPH Jane A Cecil, MD, Chris Einspahr, MSc, Betty A Forbes, PhD, Emily M. Hill, PhD, MT (ASCP), Michael P. Stevens, MD, MPH, Dan Tassone, PharmD, Leroy B. Vaughan, MD
References “Core elements of Hospital Antibiotic Stewardship Programs” https://www.cdc.gov/antibiotic-use/healthcare/implementation/core-elements.html Werner, NL, Hecker MT, Sethi AK, and Donskey CJ. “Unnecessary use of fluoroquinolone antibiotics in hospitalized patients.” BMC Infect Dis 2011; 11: 187. Kabanni S, Hersh AL, Shapiro DJ, Fleming-Dutra, Pavia AT, Hicks LA. “Opportunities to improve fluoroquinolone prescribing in the United States for Adult Ambulatory Care Visits.” Clinical Infectious Diseases. 2018; 67(1): 134–136. Lanford BJ, Seah J, Chan A, Downing M, Johnstone J, and Matukas LM. “Antimicrobial stewardship in the microbiology laboratory: impact of selective susceptibility reporting on ciprofloxacin utilization and susceptibility of gram-negative isolates to ciprofloxacin in a hospital setting.” J Clin Microbiol. 2016; 54 (0) 2343-7 Barlam TF, Cosgrove SE, Abbo LM, MacDougall C, Schuetz AN, Septimus EJ, Srinivasan A, Dellit TH, Falck-Ytter YT, Fishman NO, Hamilton CW, Jenkins TC, Lipsett PA, Malani PN, May LS, Moran GJ, Neuhauser MM, Newland JG, Ohl CA, Samore MH, Seo SK, and Trivedi KK. “Guideline for implementing an antibiotic stewardship program.” Clinical Infectious Diseases. 2016; 62(10): e51-e77. Coupat C, Pradier C, Degand N, Hofiger P, Pulcini C. “Selective reporting of antibiotic susceptibility data improves the appropriateness of intended antibiotic prescriptions in urinary tract infections: a case-vignette randomized study. Eur J Clin Microbiol Infect Dis. 2013; 32(5):627-36 Tan TY, McNulty C, Charlett A, Nesssa N, Kelly C, Beswick T. “Laboratory antibiotic susceptibility reporting and antibiotic prescribing in general practice. J. AntimicrobCemother. 2003 Feb;51(2):379-84.