Download
1 / 16
160 likes | 172 Views
Learn about adenomatous polyps, familial adenomatous polyposis (FAP), clinical features, diagnosis, treatment, and screening for large bowel cancers. Understand the different types of adenomas and their malignant potential.

E N D
THE LARGE BOWEL أعداد الدكتور زيد علي مجيد جراح اختصاص
TUMOURS OF THE LARGE INTESTINE Benign The term ‘polyp’ is a clinical description of any elevated tumour. Polyps can occur singly, synchronously in small numbers or as part of a polyposis syndrome. In familial adenomatous polyposis (FAP), more than 100 adenomas are present. It is important to be sure of the histological diagnosis because adenomas have significant malignant potential. Adenomatous polyps Adenomatous polyps vary from a tubular adenoma , rather like a raspberry on a stalk, to the villous adenoma, a flat spreading lesion. Solitary adenomas are usually found during the investigation of colonic bleeding or sometimes fortuitously. Villous tumours more usually give symptoms of diarrhoea, mucus discharge and occasionally hypokalaemia. The risk of malignancy developing in an adenoma increases with increasing size oftumour; for example, in 1-cm-diameter tubular adenomas there is a 10% risk of cancer, whereas with villous adenomas over 2cm in diameter, there may be a 15% chance of carcinoma. Adenomas larger than 5mm in diameter are usually treated because of their malignant potential. Colonoscopic snare polypectomy or diathermy obliteration with hot biopsy forceps can be used. Huge villous adenomas of the rectum can be difficult to remove even with techniques per anus, and occasionally proctectomy is required; the anal sphincter can usually be preserved. Class Varieties Inflammatory Inflammatory polyps MetaplasticMetaplastic or hyperplastic polyps HarmartomatousPeutz–Jeghers polyp , Juvenile polyp Neoplastic Adenoma – Tubular – Tubulovillous – Villous Adenocarcinoma Carcinoid tumour
Familial adenomatous polyposis FAP is clinically defined by the presence of more than 100 colorectal adenomas. Over 80% of cases come from patients with a positive family history. However, 20% arise as a result of new mutations in the adenomatous polyposis coli gene (APC). This has been identified on the short arm of chromosome 5 (Bodmer). It is less common than hereditary non-polyposis colorectal cancer (HNPCC) and accounts for less than 1% of colorectal cancer. Although the large bowel is mainly affected, polyps can occur in the stomach, duodenum and small intestine. The main risk is large bowel cancer, but duodenal and ampullarytumours have been reported. It is inherited as a Mendelian dominant condition. The risk of colorectal cancer is 100% in patients with FAP. Males and females are equally affected. It can also occur sporadically without any previous sign or history, presumably by new mutations. There is often, in these cases, a history of large bowel cancer occurring in young adulthood or middle age, suggesting pre-existing adenomatosis. FAP can be associated with benign mesodermal tumours such as desmoidtumours and osteomas. Epidermoid cysts can also occur (Gardner’s syndrome); desmoidtumours in the abdomen invade locally to involve the intestinal mesentery and, although non-metastasising, they can become unresectable . Clinical features Polyps are usually visible on sigmoidoscopy by the age of 15 years and will almost always be visible by the age of 30 years. Carcinoma of the large bowel occurs 10–20 years after the onset of the polyposis. One or more cancers will already be present in two-thirds of those patients presenting with symptoms.
Symptomatic patients These are either patients in whom a new mutation has occurred or those from an affected family who have not been screened. They may have loose stools, lower abdominal pain, weight loss, diarrhoea and the passage of blood and mucus. Polyps are seen on sigmoidoscopy, and the number and distribution of polyps, and usually cancers if they are symptomatic, are shown on a doublecontrast barium enema. If in doubt, colonoscopy is performed with biopsies to establish the number and histological type of polyps. If over 100 adenomas are present, the diagnosis can be made confidently, but it is important not to confuse this with non-neoplastic forms of polyposis. Asymptomatic patients Direct genetic testing will reveal mutations in 80% of cases. In the presence of an identified mutation in a family with FAP, any resulting negative tests for this can be interpreted to mean that these individuals do not carry the mutation. If there are no adenomas by the age of 30 years, FAP is unlikely. If the diagnosis is made during adolescence, operation is usually deferred to the age of 17 or 18 years or when symptoms or multiple polyps develop. Screening policy 1 At-risk family members are offered genetic testing in their early teens. 2 At-risk members of the family should be examined at the age of 10–12 years, repeated every year. 3 Most of those who are going to get polyps will have them at 20 years, and these require operation. 4 If there are no polyps at 20 years, continue with 5-yearly examination until age 50 years; if there are still no polyps, there is probably no inherited gene. Carcinomatous change may exceptionally occur before the age of 20 years. Examination of blood relatives, including cousins, nephews and nieces, is essential, and a family tree should be constructed and a register of affected families maintained. Treatment Colectomy with ileorectal anastomosis has in the past been the usual operation because it avoids an ileostomy in a young patient and the risks of pelvic dissection to nerve function. The rectum is subsequently cleared of polyps by snaring or fulguration. The patients are examined by flexible sigmoidoscopy at 6-monthly intervals thereafter. In spite of this, a proportion of patients develop carcinoma in the rectal stump. The risk of carcinoma in the St Mark’s series was 10% over a period of 30 years. The alternative is a restorative proctocolectomy with an ileoanal anastomosis. This has a higher complication rate than ileorectal anastomosis. It is indicated in patients with serious rectal involvement with polyps, those who are likely to be poor at attending for follow-up and those with an established cancer of the rectum or sigmoid. However, it is now used more frequently for less severe cases. There have been reports of cancers developing after stapled anastomosis when a small remnant of rectal mucosa is left behind.
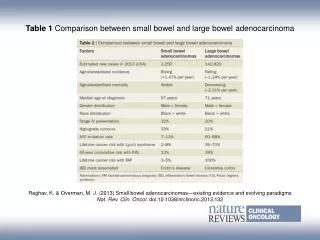
Hereditary non-polyposis colorectal cancer (Lynch’s syndrome) This syndrome is characterised by increased risk of colorectal cancer and also cancers of the endometrium, ovary, stomach and small intestines. It is an autosomal dominant condition that is caused by a mutation in one of the DNA mismatch repair genes , Most people with this syndrome have mutations in the MLH1 and MSH2 genes. The lifetime risk of developing colorectal cancer is 80%, and the mean age of diagnosis is 44 years. Most cancers develop in the proximal colon. Females with HNPCC have a 30–50% lifetime risk of developing endometrial cancer. The average age of diagnosis is 46 years in this group. Diagnosis HNPCC can be diagnosed by genetic testing or Amsterdam criteria II: • three or more family members with a HNPCC-related cancer, one of whom is a first-degree relative of the other two; • two successive affected generations; • one or more of the HNPCC-related cancers diagnosed before the age of 50 years; • exclusion of FAP. Malignant Epidemiology Colonic cancer can be diagnosed at operation as involving the large bowel proximal to where the two anti-mesenteric taenia converge (this represents the beginning of the rectum). In the UK, colorectal cancer accounted for 16000 deaths in 2003 according to Cancer Research UK statistics. It represents a large part of the general surgeon’s elective and emergency workload. Genetics There has been an explosion of information on the molecular genetics of sporadic colorectal cancer. APC mutations occur in two-thirds of colonic adenomas and carcinomas and are thought to present early in the carcinogenesis pathway. K-RAS mutations result in activation of cell signalling pathways. They are more common in larger lesions, thus implying that they are later events in the mutagenesis pathway. Other genes involved include p53. Aetiology Other factors that have been implicated in the development of cancer have included dietary fibre. The hypothesis is that increased roughage is associated with reduced transit times, and this in turn reduces the exposure of the mucosa to carcinogens. There is some evidence that links cholecystectomy, and therefore increased bile acid secretion, to an increased risk of colorectal cancer. The role of irritable bowel disease (IBD) in colorectal cancer is discussed elsewhere in this chapter.
Adenocarcinoma of the colon Pathology Microscopically, the neoplasm is a columnar cell carcinoma originating in the colonic epithelium. Macroscopically, the tumour may take one of four forms : (1) Annular; (2) tubular; (3) ulcer; (4) cauliflower The spread of carcinoma of the colon Generally this is a comparatively slow-growing neoplasm. Local spread The tumour can spread in a longitudinal, transverse or radial direction; it spreads round the intestinal wall and usually causes intestinal obstruction before it invades adjacent structures. Theulcerative type more commonly invades locally, and an internal fistula may result, for example into the bladder.
There may also be a local perforation with an abscess or even an external faecal fistula. This type of radial spread to adjacent organs has the largest impact on prognosis. The progression of invasion occurs across the submucosa into the muscularispropria and thence out into the serosa and fat, lymphatics and veins in the mesentery alongside the bowel wall. Lymphatic spread Lymph nodes draining the colon are grouped as follows: N1: nodes in the immediate vicinity of the bowel wall; N2: nodes arranged along the ileocolic, right colic, midcolic, left colic and sigmoid arteries; N3: the apical nodes around the superior and inferior mesenteric vessels where they arise from the abdominal aorta. Involvement of the lymph nodes by the tumour progresses in a gradual manner from those closest to the growth along the course of the lymphatic vessels to those placed centrally. Bloodstream spread This accounts for a large proportion (30–40%) of late deaths. Metastases are carried to the liver via the portal system, sometimes at an early stage before clinical or operative evidence is detected (occult hepatic metastases). Transcoelomic spread Rarely, colorectal cancer can spread by way of cells dislodging from the serosa of the bowel or via the subperitoneallymphatics to other structures within the peritoneal cavity. Staging colon cancer There are several staging systems that are used such as Dukes, tumour–node–metastasis (TNM) and Jass. All of them can be used in order to predict prognosis and standardise treatment. Dukes’ classification was originally described for rectal tumours (see Chapter 68) but has been adopted for histopathological reporting of colon cancer as well. There have been numerous modifications of the original system, leading to some confusion but, in its most basic form, Dukes’ classification for colon cancer is as follows: A: confined to the bowel wall; B: through the bowel wall but not involving the free peritoneal serosal surface; C: lymph nodes involved. Dukes himself never described a D stage, but this is often used to describe either advanced local disease or metastases to the liver.
TNM classification The TNM classification is more detailed and accurate but more demanding: • T Tumour stage; • T1 Into submucosa; • T2 Into muscularispropria; • T3 Into pericolic fat but not breaching serosa; • T4 Breaches serosa or directly involving another organ; • N Nodal stage; • N0 No nodes involved; • N1 One or two nodes involved; • N2 Three or more nodes involved; • M Metastases; • M0 No metastases; • M1 Metastases; • Ly Lymphatic invasion; • L0 No lymphatic vessels involved; • L1 Lymphatics involved; • V Venous invasion; • V0 No vessel invasion; • V1 Vessels invaded; • R Residual tumour; • R0 No residual tumour; • R1 Margins involved, residual tumour present. Clinical features Carcinoma of the colon usually occurs in patients over 50 years of age, but it is not rare earlier in adult life. Twenty per cent of cases present as an emergency with intestinal obstruction or peritonitis. In any case of colonic bleeding in patients over the age of 40 years, a complete investigation of the colon is required. A careful family history should be taken. Those with first-degree relatives who have developed colorectal cancer at the age of 45 years or below are at high risk and may be part of one of the colorectal cancer family syndromes.
Carcinoma of the left side of the colon Most tumours occur in this location. They are usually of the stenosing variety. Symptoms The main symptoms are those of increasing intestinal obstruction. This includes lower abdominal pain, which may be colicky in nature, and abdominal distension. The patient may have a change in bowel habit with alternating diarrhoea and constipation . Symptoms and signs of colorectal cancer ■ Right-sided tumours: iron deficiency anaemia, abdominal mass ■ Left-sided tumours: rectal bleeding, alteration in bowel habit, tenesmus, obstruction ■ Metastatic disease: jaundice, ascites, hepatomegaly; other symptoms and signs from rarer sites of metastasis ■ There may be considerable overlap between these symptoms Carcinoma of the sigmoid In addition to symptoms of intestinal obstruction, a low tumour may give rise to a feeling of the need for evacuation, which may result in tenesmus accompanied by the passage of mucus and blood. Bladder symptoms are not unusual and, in some instances, may herald a colovesical fistula. Carcinoma of the transverse colon This may be mistaken for a carcinoma of the stomach because of the position of the tumour together with anaemia and lassitude Carcinoma of the caecum and ascending colon This may present with the following: • anaemia, severe and unyielding to treatment; • the presence of a mass in the right iliac fossa; colonoscopy may be needed to confirm the diagnosis; • a carcinoma of the caecum can be the apex of an intussusception presenting with the symptoms of intermittent obstruction. Methods of investigation of colon cancer Flexible sigmoidoscopy The 60-cm, fibreoptic, flexible sigmoidoscope is increasingly being used in the out-patient clinic or in special rectal bleeding clinics.
Colonoscopy This is now the investigation of choice if colorectal cancer is suspected provided the patient is fit enough to undergo the bowel preparation. Radiology Double-contrast barium enema is used when colonoscopy is contraindicated. It shows a cancer of the colon as a constant irregular filling defect , Ultrasonography is often used as a screening investigation for liver metastases over the size of 1.5cm, and CT is used in patients with large palpable abdominal masses, to determine local invasion, and is particularly used in the pelvis in the assessment of rectal cancer. Urograms have a role in left-sided tumours where there is evidence of hydronephrosis on CT or ultrasound.
Enterocutaneous or faecalfistula An external fistula communicating with the caecum sometimes follows an operation for gangrenous appendicitis or the draining of an appendix abscess. A faecal fistula can occur from necrosis of a gangrenous patch of intestine after the relief of a strangulated hernia, or from a leak from an intestinal anastomosis. The opening of an abscess connected with chronic diverticulitis or carcinoma of the colon frequently results in a faecal fistula. Radiation damage is also another cause of fistula formation. The most common cause of enterocutaneous fistula is, however, previous surgery. This happens most often in patients with adhesions following previous operations. Damage to the small intestine occurs inadvertently during dissection of the adhesions and, because of an associated subacute obstruction or abscess, the fistula ‘blows’ postoperatively. Enterocutaneous fistulae can be divided into: • those with a high output, more than 1 litre day–1; • those with a low output, less than 1 litre day–1. They can also be described anatomically as simple, with a direct communication between the gut and the skin, or complex, i.e. those with one or more tracts that are tortuous and sometimes associated with an intervening abscess cavity half way along the tract. The discharge from a fistula connected with the duodenum or jejunum is bile-stained and causes severe excoriation of the skin. When the ileum or caecum is involved, the discharge is fluid faecal matter; when the distal colon is the affected site, it is solid or semisolid faecal matter. The site of leakage and the length of the fistula can be determined by small bowel enema and barium enema, by fistulography and, most importantly, by CT of the abdomen will show up any associated abscesses . Treatment This can be very challenging in patients with a high-output fistula. Low-output fistulae can be expected to heal spontaneously, provided there is no distal obstruction. Reasons for failure of spontaneous healing also include: • epithelial continuity between the gut and the skin; • the presence of active disease where, for example, there is CD or carcinoma at the site of the anastomosis or in the tract; • an associated complex abscess. The abdominal wall must be protected from erosion by the use of appliances. The patient must remain nil by mouth; intravenous nutrition is started and signs of a decrease in fistula output are sought.
The higher the fistula in the intestinal tract, the more skin excoriation must be expected, and this is worst in the case of a duodenal fistula. High-output fistulae cause rapid dehydration and hypoproteinaemia. Vigorous fluid replacement and nutritional support are essential. The drainage of an intra-abdominal abscess can be life-saving. This can be achieved by either CT-guided drainage or, occasionally, laparotomy. In patients with a complex fistula, it may be necessary to bring out a defunctioning stoma upstream of the fistula site, even if this results in a high-output stoma. Operative treatment Operative repair should be attempted only after a trial of conservative management. The surgery can on occasion be extremely technically demanding, and an anastomosis should not be fashioned in the presence of continuing intra-abdominal sepsis or when the patient is hypoproteinaemic. STOMAS ColostomyA colostomy is an artificial opening made in the large bowel to divert faeces and flatus to the exterior, where it can be collected in an external appliance. Depending on the purpose for which the diversion has been necessary, a colostomy may be temporary or permanent. Temporary colostomy A transverse loop colostomy has in the past been most commonly used to defunction an anastomosis after an anterior resection. It is now less commonly employed as it is fraught with complications and is difficult to manage; a loop ileostomy is preferred. A loop left iliac fossa colostomy is still sometimes used to prevent faecal peritonitis developing following traumatic injury to the rectum, to facilitate the operative treatment of a high fistulain-ano and incontinence. A temporary loop colostomy is made, bringing a loop of colon to the surface, where it is held in place by a plastic bridge passed through the mesentery. Once the abdomen has been closed, the colostomy is opened, and the edges of the colonic incision are sutured to the adjacent skin margin . When firm adhesion of the colostomy to the abdominal wall has taken place, the bridge can be removed after 7 days. Following the surgical cure or healing of the distal lesion for which the temporary stoma was constructed, the colostomy can be closed. It is usual to perform a contrast examination (distal loopogram) to check that there is no distal obstruction or continuing problem at the site of previous surgery. Colostomy closure is most easily and safely accomplished if the stoma is mature, i.e. after the colostomy has been established for 2 months. Closure is usually performed by an intraperitoneal technique, which is associated with fewer closure breakdowns with faecal fistulae. Double-barrelled colostomy This colostomy was designed so that it could be closed by crushing the intervening ‘spur’ using an enterotome or a stapling device. It is rarely used now, but occasionally the colon is divided so that both ends can be brought to the surface separately, ensuring that the distal segment is completely defunctioned. Permanent colostomy This is usually formed after excision of the rectum for a carcinoma by the abdominoperineal technique. It is formed by bringing the distal end (end-colostomy) of the divided colon to the surface in the left iliac fossa, where it is sutured in place, joining the colonic margin to the surrounding skin.
The point at which the colon is brought to the surface must be carefully selected to allow a colostomy bag to be applied without impinging on the bony prominence of the anterosuperior iliac spine. The best site is usually through the lateral edge of the rectus sheath, 6cm above and medial to the bony prominence . Closure of the lateral space between the intraperitoneal segment of the sigmoid colon and the peritoneum of the pelvic wall, to prevent internal herniation or strangulation of loops of small bowel through the deficiency, has been practised, but there is no good evidence that it is effective. Colostomy bags and appliances Faeces from a permanent colostomy are collected in disposable adhesive bags. A wide range of such bags is currently available. Many now incorporate a stomahesive backing, which can be left in place for several days. In most hospitals, a stoma care service is available to offer advice to patients, to acquaint them with the latest appliances and to provide the appropriate psychological and practical help. Complications of colostomies The following complications can occur to any colostomy but are more common after poor technique or siting of the stoma: • prolapse; • retraction; • necrosis of the distal end; • fistula formation; • stenosis of the orifice; • colostomy hernia; • bleeding (usually from granulomas around the margin of the colostomy); • colostomy ‘diarrhoea’: this is usually an infective enteritis and will respond to oral metronidazole 200 mg three times daily. Many of these complications require revision of the colostomy. Sometimes, this can be achieved with an incision immediately around the stoma but, on occasion, reopening the abdomen and freeing up the colostomy may be necessary. Occasionally, transfer to the opposite side of the abdomen may be necessary. Loop ileostomy An ileostomy is now often used as an alternative to colostomy, particularly for defunctioning a low rectal anastomosis. The creation of a loop ileostomy from a knuckle of terminal ileum has already been described. The advantages of a loop ileostomy over a loop colostomy are the ease with which the bowel can be brought to the surface and the absence of odour. Care is needed, when the ileostomy is closed, that suture line obstruction does not occur. Caecostomy This is rarely used now. In desperately ill patients with advanced obstruction, a caecostomy may be useful. In late cases of obstruction, the caecum may become so distended and ischaemic that rupture of the caecal wall may be anticipated. This can occur spontaneously, giving rise to faecal peritonitis, or at operation, when an incision in the abdominal wall reduces its supportive role and allows the caecum to expand.
In such a situation, it should be decompressed by suction as soon as the abdomen is opened. In thin patients, it may then be possible to carry out direct suture of the incised or perforated caecal wall to the abdominal skin of the right iliac fossa, although a resection of this area is really the best treatment. Following on-table lavage, via the appendix stump, the irrigating catheter can be left in place as a tube caecostomy. Caecostomy is only a short-term measure to allow a few days for the condition of the patient to improve. Reoperation should normally follow soon thereafter and a definitive procedure should be carried out.