Download
1 / 31
480 likes | 1k Views
EKG for ACLS. Amanda Hooper 2008-2009. Let’s start with some basics…. V1: right 4 th intercostal space V2: left 4 th intercostal space V3: halfway between V2 and V4 V4: left 5 th intercostal space, mid-clavicular line V5: horizontal to V4, anterior axillary line

E N D
EKG for ACLS Amanda Hooper 2008-2009
Let’s start with some basics… • V1: right 4th intercostal space • V2: left 4th intercostal space • V3: halfway between V2 and V4 • V4: left 5th intercostal space, mid-clavicular line • V5: horizontal to V4, anterior axillary line • V6: horizontal to V5, mid-axillar line
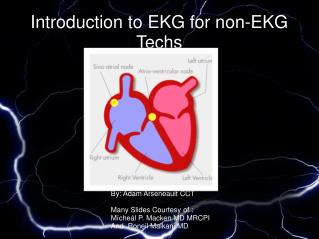
Conduction System of the Heart • Sinus node is the pacemaker of the heart, the dominant center of automaticity. • Generates continuous regular depolarization stimuli at a rate of 60-100 bpm • There are other potential pacemakers that can take over if SA node fails, and they have different intrinsic rates. These are in the atria, AV junction, and the ventricles.
EKG Paper • EKG machine moves at 25 mm/sec, each small box is 1 mm • Small boxes represent 0.04 sec • Large boxes represent 0.2 sec • Five large boxes equal one second
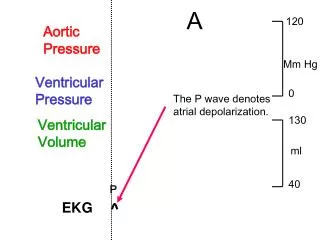
EKG Waves and Intervals • P wave: the sequential activation (depolarization) of the right and left atria • QRS complex: right and left ventricular depolarization (normally the ventricles are activated simultaneously) • ST-T wave: ventricular repolarization • PR interval: time interval from onset of atrial depolarization (P wave) to onset of ventricular depolarization (QRS complex) • QRS duration: duration of ventricular muscle depolarization • QT interval: duration of ventricular depolarization and repolarization
Systematic Approach to ECG Interpretation • Rate • Rhythm • Axis • Intervals • Hypertrophy • Infarct (QRST Changes)
Determining Rate • R-R interval is ventricular rate • p-p interval is atrial rate. Usually the same but not always • Several ways to do this… • 1) Count down the number of large boxes: 300, 150, 100, 75, 60, 50, .... • Ex: this one is between 150 and 100, closer to 150 so we might say ~130-140 bpm • 2) Count the number of large boxes and divide by 300 • Ex: 300/2 = 150 but it is a little slower than that so we might say ~130-140 bpm • 3) Count the number of small boxes between beats and divide into 1500 • Ex: 1500/11 = 136 bpm
Analyzing A Rhythm Strip • Is the rhythm regular? • What is the rate? • Is the QRS complex narrow or wide? • Are P waves present? • Are P waves related to the QRS complexes? • What is the PR interval ?
Intervals • PR interval • From the onset of atrial depolarization to the onset of ventricular depolarization • Normal between 0.12 and 0.20 sec—so should be less than a large box • QRS interval: • Time it takes for ventricular depolarization to occur • Normal is 0.10 sec or less—so should be less than half of a large box • QT interval • From the beginning of ventricular depolarization to the end of ventricular repolarization • Normal is les than half of a R-R interval (can’t always rely on this if rate is very tachycardic)
Supraventricular Tachycardia (SVT) • Supraventricular rhythms start by definition at or above the AV node. If the QRS is narrow in all leads, you can almost be guaranteed the rhythm is supraventricular. • Sinus rhythm, atrial fibrillation, atrial flutter, junctional/nodal rhythms, and PSVT • PSVT is a reentry rhythm
Myocardial Infarction • Look for QRST changes in each lead • Note each lead where Q waves are found • Look for R wave progression—transition normally occurs between V2 and V4 • Look at ST segments and note depression or elevation • Look for T wave inversion • Q waves or T wave inversion may be a normal finding in leads III, aVF, aVL, aVR, and V1
Basic Lead Groupings • Inferior leads: II, III, aVF • Lateral (left-sided) leads: V4 to V6 and I, aVL • Septal leads: V1, V2 • Anterior leads: V2 to V4 • Right coronary artery: • SA node, IV septum, inferior heart, +/- posterior heart • Left coronary artery: • LAD- anterior heart • Left circumflex- lateral heart
Inferior MI with RV Infarction From: Heart Disease 6th Edition. Braunwald E, Zipes D, and Libby P. 2001