Download
1 / 1
10 likes | 115 Views
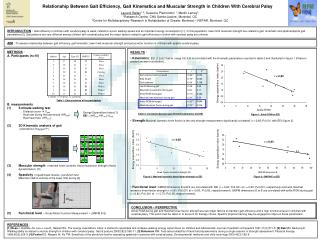
Relationship Between Gait Efficiency, Gait Kinematics and Muscular Strength in Children With Cerebral Palsy. Laurent Ballaz 1, 2 ; Suzanne Plamondon 1 ; Martin Lemay 1 ; 1 Research Centre, CHU Sainte-Justine, Montréal, QC

E N D
Relationship Between Gait Efficiency, Gait Kinematics and Muscular Strength in Children With Cerebral Palsy Laurent Ballaz1, 2; Suzanne Plamondon 1; Martin Lemay1; 1Research Centre, CHU Sainte-Justine, Montréal, QC 2Centre for Multidisciplinary Research in Rehabiliation of Greater Montreal – REPAR, Montreal, QC INTRODUCTION:Gait efficiency in children with cerebral palsy is weak, related to a poor walking speed and an important energy consumption [1] . In this population, lower limb muscular strength are related to gait kinematic and spatiotemporal gait parameters [2]. Gait patterns are very different among children with cerebral palsy and the major factors related to gait efficiency in cildren with cerebral palsy are unknow. AIM: To assess relationship between gait efficiency, gait kinematic, lower limb muscular strength and gross motor function in children with spastic cerebral palsy. • METHODS: A. Participants (n=10) • B. measurements • 5-minute walking test Distance cover Vwalk Heat rate during the last minute (HRwalk) Rest heart rate (HRrest) • 3D Kinematic analysis of gait • (VICON 512; Polygon™) • Muscular strength : maximal knee isométric flexion/extension strength (Hand dynamometer) [3] • Spasticityof quadriceps muscle : pendulum test • Maximal rotation velocity of the lower limb during [4] • Functional level « Gross Motor Function Measurement » (GMFM D-E) • RÉSULTS : • Kinematics: EEI (1,5±0,7 bat/m, range 0,6-2,6) is correlated with the kinematic parameters reported in table 2 and illustrated in figure 1 (Pearson product moment correlation),. • Strength:Maximal isometric knee flexion is the only strength measurement significantly correlated (r =-0,85;P<0,01) with EEI (figure 2). • Functional level: GMFM dimensions D and E are correlated with EEI (r =-0,94; P<0,001 et r =-0,80; P<0,001, respectively) and with maximal isometric knee flexion strength (r =0,91; P<0,001 et r =0,93; P<0,05, respectivement). GMFM dimensions D et E are correlated with ankle ROM during gait (r =0,82; P<0,001 et r = 0,73; P<0,05, respectivement). Energy expenditure index (bat/m) r =-0,82 D, diplegia; H, hemiplegia; Q, quadriplegia Table 1: Characteristics of the participants Ankle ROM Energy Expenditure Index [1] EEI = (HRwalk-HRrest)/Vwalk Table 2: correlation between gait kinematic parameter and EEI Figure 1: Ankle ROM vs EEI r =-0,85 r =-0,80 Energy expenditure index (bat/m) Energy expenditure index (bat/m) Knee flexion isometric strength (N) GMFM dimension E Figure 2: Maximal isometric knee flexion strength vs EEI Figure 3: GMFM-E vs EEI ωmax CONCLUSION – PERSPECTIVE Ankle ROM during gait and maximal knee flexion strength are two major factors to maintain gait efficiency and a high fonctional level in children with cerebral palsy. This point must be taken in to account for therapy choice. Specific physical training may be engaged to improve these parameters. REFERENCES: [1] Rose J, Gamble JG, Lee J, Lee R, Haskell WL. The energy expenditure index: a method to quantitate and compare walking energy expenditure for children and adolescents. Journal of pediatric orthopedics 1991;11(5):571-8. [2] Eek MN, Beckung E. Walking ability is related to muscle strength in children with cerebral palsy. Gait & posture 2008;28(3):366-71. [3] Bohannon RW. Test-retest reliability of hand-held dynamometry during a single session of strength assessment. Physical therapy 1986;66(2):206-9.[4] Fowler EG, Nwigwe AI, Ho TW. Sensitivity of the pendulum test for assessing spasticity in persons with cerebral palsy. Developmental medicine and child neurology 2000;42(3):182-9.