Download
1 / 40
400 likes | 421 Views
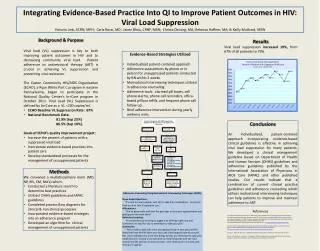
Explore the integration of evidence, values, and ethics in healthcare decision-making from policy to practice, focusing on ethical considerations and conflicting interests in a physician's role. Delve into the challenges and guidelines for treating rare conditions such as Prader-Willi Syndrome, emphasizing the importance of universal healthcare access, ethical medical practices, and patient-centered care. Learn from historical perspectives like the Hippocratic Oath and modern medical research in growth hormone deficiencies.

E N D
Integrating Evidence, Values and Ethics from Policy to Practice: A Multicriteria Reflection The View of a Practicing Physician Cheri L. Deal, Ph.D., M.D. Chief, Endocrine and Diabetes Service, CHU- Ste-Justine Professor of Pediatrics, Université de Montréal
Recent/Ongoing Research Contracts - Lilly, Merck-EMD Serono, Sandoz, Versartis Continuing Medical Education Grants - Lilly, Merck-EMD Serono, Sandoz, Pfizer, Hoffmann- La Roche Ad hoc Consulting - Lilly, Merck-EMD Serono, Pfizer, Sandoz, Novo-Nordisk, Hoffmann-LaRoche, Versartis, Prolor Invited Speaker and/or Chairperson for Symposia sponsored by: Lilly, Merck-EMD Serono, Pfizer, Sandoz, Novo-Nordisk CONFLICTS OF INTEREST/BIASES
‘Children represent the future, and ensuring their healthy growth and development ought to be a prime concern of all societies’ BIASES and BELIEFS Access to universal healthcare Address contextual factors to ill health: social, economic and environmental Access to medical products
Outline • Reflections on Hippocrates • Brief medical history of Prader-Willi Syndrome, and the use of Growth Hormone (GH) • Why evidence for GH treatment in this population is very difficult to obtain, assess and act upon • The GRS International Consensus Guidelines Publication and MCDA Deal et al, J ClinEndocrinolMetab, 2013
Hippocratic OathI will swear to fulfill, to the best of my ability and judgement: I will respect the hard-won scientific gains of those physicians in whose steps I walk, and gladly share such knowledge as is mine with those who are to follow. I will apply, for the benefit of the sick, all measures which are required, avoiding those twin traps of overtreatment and therapeutic nihilism. I will remember that there is art to medicine as well as science, and that warmth, sympathy, and understanding may outweigh the surgeon's knife or the chemist's drug. I will not be ashamed to say "I know not," nor will I fail to call in my colleagues when the skills of another are needed for a patient's recovery.
I will respect the privacy of my patients, for their problems are not disclosed to me that the world may know. Most especially must I tread with care in matters of life and death. If it is given me to save a life, all thanks. But it may also be within my power to take a life; this awesome responsibility must be faced with great humbleness and awareness of my own frailty. Above all, I must not play at God. I will remember that I do not treat a fever chart, a cancerous growth, but a sick human being, whose illness may affect the person's family and economic stability. My responsibility includes these related problems, if I am to care adequately for the sick. I will prevent disease whenever I can, for prevention is preferable to cure. I will remember that I remain a member of society, with special obligations to all my fellow human beings, those sound of mind and body as well as the infirm.
At 18 y: BMI=47; 263% IBW Ht=140 cm At 16 y BMI=59; 307% IBW Ht=156 cm
Height Weight BOYS GIRLS de Sanctis V: Manual of Growth Charts and Body Standard Measurements, 2nd ed. Pacini ed, S.p.A., Pisa, 2001. p 83-84. Data from: Butler MG, Meaney FJ: Standards for selected anthropometric measurements in PWS. Pediatrics 88:853, 1989.
Prader-Willi Syndrome • Pre- and post-natal hypotonia • Weak cry, poor suck, failure to thrive • Characteristic facial features • Obesity syndrome with hyperphagia • Hypogonadism with LH/FSH deficiency • Short adult stature with GH deficiency • Potential TSH and ACTH deficiency • Global developmental delay, intellectual disability (IQ 70-80), behavioural problems ± epilepsy, ± psychiatric phenotypes
Patients with PWS Are Not All The Same! • Growth and GH status • Dysmorphic features • Obesity and body composition • Metabolic profile • Sleep • Breathing • Scoliosis • Psychomotor development and cognitive aspects • Behavioral phenotype (food-seeking) • Mortality • Not entirely due to the different • genetic causes of PWS • Bckg genetics, environments differ Cassidy et al, Am J Med Genet, 1997; Whittington et al, J Dis Res, 2004; Varela et al, Clin Genet, 2005; Theodoro et al, Obesity, 2006; Torado et al, Am J Med Genet, 2007; Lin et al, Acta Paediatr, 2007; Odent et al, Pediatrics, 2008; Williams et al, J Clin Sleep Med, 2008; Holsen et al, Int. J Obesity, 2009; Grugni et al, J Endocrinol Invest, 2011; Sinnema et al, Res Dev Disabil, 2011
Growth Hormone History in PWS: Evidence for GH Defiency • Low GH response to pharmacologic stimuli • Parra et al, 1973; Bray et al 1980 • Low levels of IGF-I, IGF-II and IGFBP-3, despite obesity • Lee et al, 1987, Costeff et al, 1990, Thacker et al, 1998 • Initial GH treatment data in children • Lee et al, 1987, n=4 • Clinical research center study of endocrine function and GH therapy in children • Lee et al, 1992
GH History in PWS, cont. • European GH studies in children • Eiholzer; Ritzén & Lindgren, 1990s • US controlled trial of GH in childhood PWS • Carrel et al, 1999 – randomized control, 1y Tx • The FIRST randomized, double-blind, cross-over • design, placebo-controlled trialof GH therapy • in PWS children published in 2003 (6 months) Effects on Growth, Body Composition, Pulmonary Function, Behaviour Haqq et al, J Clin Endocrinol Metab, 2003
GH History in PWS, cont. • US FDA ‘Orphan Drug’ labeling of GH for childhood • PWS (2000) • European labeling of GH for childhood PWS (2006) • Australian labeling of GH for childhood PWS (2008) FACTS: - GH therapy is expensive (5,000-30,000$/year) and must be given by subcutaneous injection - PWS support groups world-wide argue for its use
Data on GH in PWS After Regulatory Approval • GH trials (control groups now on GH), long term • InfantCarrel et al, 2010 – 6y Tx • Childhood de Lind van Wijngaarden et al, 2009 – 4y Tx • Adult Höybye et al, 2007 – 5y Tx • GH randomized, placebo-controlled studies in adults • 6 months Höybye et al, 2003 • 12 monthsSode-Carleson et al, 2010 • Registry data: Pfizer (n=2151), Genentech (n=564), • NovoNordisk (n=137), Lilly (n=112), • Meta-analysis, GH use in PWS • Craig, Johnston, Cowell, Cochrane Reviews, in review • -Sanchez-Ortiga, Klibanski, Tritos, ClinEndocrinol, 2011
Side Effects Based on Conditions of GH Excess (Acromegaly), and/or Theoretical Considerations and/or Reported Adverse Events in Patients Treated with GH (PWS and others) Sleep apnea Sudden death Scoliosis Glucose intolerance, Diabetes Intracranial hypertension Epilepsy Slipped capital femoral epiphyses Risk of infection Joint pain, Oedema Gynecomastia • (Neoplasia) – bone tumors, meningioma, other solid tumors • (data from NON-PWS patients) • (Arterial Hypertension, Stroke/intra-cranial bleeding)
Sudden Death and GH Safety N=1+2 GH Tx= No GH-Tx, BUT 75% of GH-treated patients died with 9 months of GH start
Beyond Stature: Clinical Characteristics of PWS Potentially Benefiting from GH Therapy • Hypotonia • Delayed motor development • Obesity with low energy expenditure • Increased body fat • Decreased muscle mass • Reduced exercise tolerance • Metabolic syndrome • Osteoporosis • Impaired cognitive function
My Dilemma with HTA within the Context of Rare Diseases such as PWS, and GH Treatment • Imperfect evidence: study biases • Population with intellectual disabilities • Genetic heterogeneity • Safety concerns around GH • Clinical observations in the real world • Clinical goals of physicians at odds with the basis for GH approval: metabolic outcome versus growth • Cost of drug not seen in the larger perspective of the cost of overall care of patients and theirfamilies living with PWS
Nutrition Counselling Speech Therapy O.T. P.T. Neurology FU Psychology FU Psychiatry FU Endocrinology FU GH Dental Clinic Sleep Clinic Orthopedics FU Ophthamology FU
GRS International Clinical Care Guidelines Workshop on GH and Prader-Willi Syndrome: Montreal, October 2011 Funded by: Growth Hormone Research Society Prader-Willi Research Foundation EVIDEM 22
Why The Workshop No ‘formal’ consensus guidelines for GH and PWS, other than 2006 Toulouse Workshop Sponsored by one pharmaceutical company JCEM 2008 Guidelines from this Expert Meeting GH therapy only a small section of the document No attempt to grade the level of evidence Based on mostly observational (level II B,C or D) and on 2 randomized, controlled trials, moderate evidence only, due to confounders (level IB)
Format 3-day meeting Oct 3-7, 2011 43 PWS experts, including: - Pediatric and Adult Endocrinologists - Geneticists (clinical and basic) - Clinicians and Scientists with interest growth hormone research (GRS Council Members) - PWS Patient Advocate USA/Canada - Bioethicist - Orthopedic Surgeon - Psychiatrist - Methodologists (epidemiology, health technology evaluation - Health Economist (Economics of Obesity)
Organising Committee:Cheri Deal (Canada), Jens Christiansen (Denmark), Maithe Tauber (France), Charlotte Höybye (Sweden), David Allen (USA)
Multi-Criteria Healthcare Decision-Making Scientific Considerations Contextual Considerations Disease impact • Disease severity, Size of affected population Context of intervention • Clinical guidelines, Comparative intervention Intervention outcomes • Improvement of efficacy/effectiveness • Improvement of safety and tolerability • Improvement of patient reported outcomes Type of benefit • Public health interest (prevention, risk reduction) • Type of medical service (symptom relief, cure) Economics • Budget impact (cost of intervention only) • Impact on other spending (hospitalization, disability) • Cost-effectiveness of intervention Quality/uncertainty of evidence • Adherence to requirements of decisionmaking body • Completeness and consistency of reporting evidence • Relevance and validity of evidence Ethical framework • Goals of healthcare - utility • Opportunity costs – efficiency • Population priority & access – issues of fairness Other system related criteria • System capacity and appropriate use of intervention • Stakeholder pressures • Political/historical context
Working Groups Answered (in writing, with references) Specific Questions Using MCDA Framework Example:
Sample Questions, cont. Example:
Questions, cont. Example:
Systematic literature reviewof PubMed, EMBASE, Cochrane Reviews, Controlled Trials Registries and government and HTA agency websites; these were completed by hand searching of bibliographies. • Pediatric AND adult publications included:randomized controlled trials, comparative observational studies and uncontrolled trials, longer term studies (>3.5 years in kids; ≥ 6 months in adults) • Summaries produced for relevant studies and posted on the web http://www.evidem.org/ • Level of evidencewas evaluated using the scoring procedure based on the Oxford Centre for Evidence-based Medicine Level of Evidence scale (1 to 5); Level of recommendation graded from Best (A) to Worst (D) • 5 companies provided safety data (registry/SAE): Pfizer, Genentech, Lilly, Novo Nordisk, Serono
Web-based Evidence Tables and Grading http://www.evidem.org/praderwilli.
Summaries Produced for Relevant Studies (Clinical Trials with Control Group) METHODOLOGY ARTICLE PDF
Sources of Bias: A Reality • No placebo; investigators and families not blinded • Randomization procedure not discussed • Sample sizes small: no stratification by genotype • Confounding variables • inconsistent documentation of food intake • inconsistent documentation of activity level • minimal data on psychosocial setting: • parental education, income, employment • Inconsistent use of intention to treat analyses • Incomplete reporting of patient numbers • Limited statistical details (p-values only) • Rare reporting of individual patient responses
Recommendations JCEM, 2013 After genetic confirmation of the diagnosis of PWS, GH treatmentshould be considered and, if initiated, continued for as long as demonstrated benefits outweigh the risks. Recommendation A; evidence 1
164A:671-675, 2014 • 14 patients (10 DEL, 4 UPD) • GH Start 11.9 y (7.1-14.1) • GH Stop 15.6 y (14.0-17.9) • Duration Tx 4.0 y (1.8-8.8) Visceral Fat BMI-SDS Subcutaneous Fat -24 m +24 m
More Data on Developmental and Cognitive Impact Siemensma et al, J Clin Endocrinol Metab, 97:2307, 2012 N=22 N=48 Reus et al, Res in Develop Disabilities, 34:3092, 2013
164A:2226-2231, 2014 • First to study QoL in primary caregivers of patients with PWS • Questionnaires, 5 domains: • Physical, Psychological, Social, Environmental, QoL Impression • Group effects studied: • -Deletion (32) vs UPD (13) • -Children 6-12 y (22) vs Adolescents 13-19 y (23) • Results show deterioration of QoL at adolescence with caregivers of UPD patients particularly affected
Conclusions • Evaluations of therapeutic interventions for rare diseases remind me of Montreal streets: full of potholes • MCDA can help us to avoid and/or fill them, using a systematic, structured approach • MCDA is useful as a framework for asking the right questions in CPG guidelines and for understanding an individual’s priorities
Concerning Budget Considerations for Unmet Needs in Rare Diseases… If it’s your car falling in the pothole, will you really be able to say that you understand why it hasn’t been filled?
Special Thanks To MY PATIENTS The Workshop Organising Committee :Jens Christiansen (Denmark), Maithe Tauber (France), Charlotte Höybye (Sweden), David Allen (USA) The GRS :John Kopchick, President (USA), Beverly Biller (USA), Gudmundur Johannsson (Sweden), Hassy Cohen (USA), Sally Radovick (USA), Mike Waters (Australia), Kazuo Chihara (Japan) Workshop Attendees: • Maria Craig (Australia) • Rob Nicholls (USA) • Alex Kemper (USA) • Geoff Ambler (Australia) • Sara Rosenthal (USA) • Tiziana Greggi (ITALY) • Jennifer Miller (USA) • Merlin Butler (USA) • Suzanne Cassidy (USA) • Graziano Grugni (Italy) • Ricard Nergardh (Sweden) • Ilkka Sipilä (Finland) • Jean-Eric Tarride (Canada) • Anita Hokken-Koelega (NL) • Hariette Mogul (USA) • Françoise Muscatelli (France) • Michèle Tony (Canada) • Saul Malozowski (USA) • Glen Berall (Canada) • Véronique Beauloye (France) • Tony Goldstone (UK) • Annick Vogels (Belgium) • Renaldo Battista (Canada) • Keegan Johnson (PWS USA/Canada) • Mireille Goetghebeur (EVIDEM, Canada) • Drs. Quigley, Kappelgaard, Wollmann, Lippe, Haahr