Download
1 / 111
1.17k likes | 1.69k Views
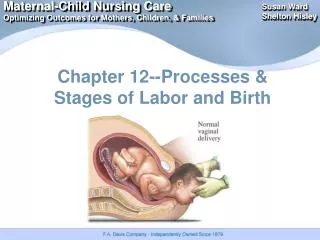
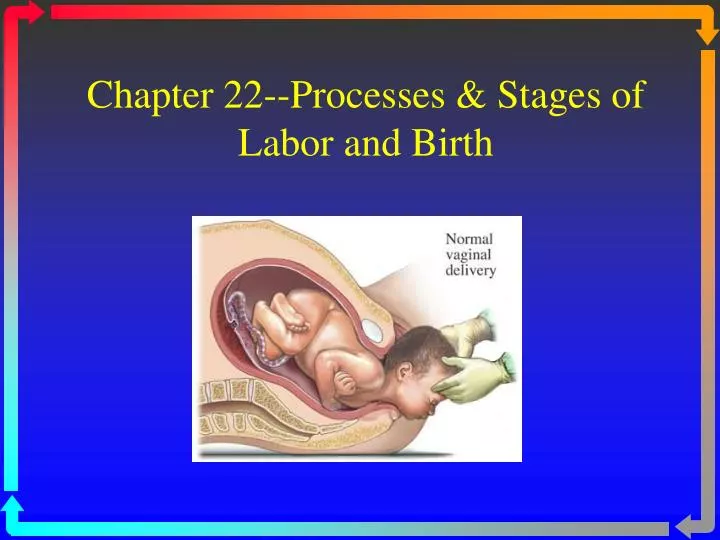
Chapter 22--Processes & Stages of Labor and Birth. Critical Factors In Labor. The Four P’s: passage, passenger, powers & psyche Passage : adequate pelvis? cephalopelvic disproportion (CPD) Suspect if presenting part does not engage in pelvis (0 station). Passenger.

E N D
Critical Factors In Labor • The Four P’s: passage, passenger, powers & psyche • Passage: • adequate pelvis? • cephalopelvic disproportion (CPD) • Suspect if presenting part does not engage in pelvis (0 station)
Passenger • The fetus: head is largest diameter • Fetal head: 4 bones with 3 membranous interspaces (sutures) that allow bones to move & overlap to diminish size of skull • Molding: head becomes narrower, longer, sutures can overlap--normal--resolves 1-2 days after birth • Fontanelles: at junctures of skull bones
Fetal Lie and Presentation • Leopold's maneuvers/US • Longitudinal lie: Vertical • Presenting part: • cephalic (head), • vertex (occiput), chin (mentum) • breech (buttocks or feet) (c-section) • sacrum • Transverse lie: Horizontal (c-section) • Presenting part: shoulder (acromion)
Fetal position: • mom’s pelvis is divided into 4 quadrants: RA, RP, LA, LP • determine which quadrant presenting part (occiput) is pointing towards
Passenger • Occiput Anterior (LOA & ROA): most common positions & easiest for birth • Occiput Posterior (LOP & ROP): • can prolong both 1st & 2nd stage of labor • back pain during UCs (back labor) • Instruct partner in sacral pressure during UC’s • Try “all fours,” knee-chest, or alternate side-lying positions to encourage baby to rotate to anterior position
Powers • Contractions: supplied by fundus of uterus • Involuntary, become stronger as labor progresses • Abdominal muscles: “pushing” by mom (2nd stage) Psyche • Psychological state & feelings of mom • Coping skills • Anxiety, fear, stress • Labor support
Onset of labor • Usually begins between 38 & 42 weeks • Mechanism is unknown • Upper uterus contracts downward pushing presenting part on cervix causing effacement and dilatation • Premonitory signs of labor: • Lightening, Braxton-Hicks contractions (false labor), • cervical changes (ripening), • bloody show (mucous plug), • rupture of membranes (ROM), • sudden burst of energy
False Labor Benign and irregular contractions Felt first abdominally and remain confined to the abdomen and groin Often disappear with ambulation and sleep. Do not increase in duration, frequency or intensity True Labor: Begin irregularly but become regular and predictable Felt first in lower back and sweep around to the abdomen in a wave Continue no matter what the women’s level of activity Increase in duration, frequency, and intensity False vs True Labor:Contractions
False Labor No significant change in dilation or effacement No significant bloody show Fetus- presenting part is not engaged in pelvis True Labor Progressive change in dilation and effacement Bloody show Presenting part engages in pelvis False vs True Labor:Cervix
Critical Thinking • A primigravida client has just arrived in the birthing unit. What steps would be most important for the nurse to perform to gain an understanding of the physical status of the client and her fetus? A. Check for ruptured membranes, and apply a fetal scalp electrode B. Auscultate the fetal heart rate between and during contractions C. Palpate contractions and resting uterine tone D. Perform a vaginal exam for cervical dilation, and perform Leopold's maneuvers E. Determine gestational age of fetus
Stages of Labor: First Stage • 0 to 10 cm: dilatation--opening of cervix) • Latent: slowest part of the process--slow dilation, mild contractions • from onset of regular UCs to rapid dilatation (about 3-4 cms) • Active: labor “picks up steam”--period of more rapid dilation • from 4 cm to full dilatation: stronger UCs • Transition: 7-10 cm--intense, N/V, shaking
Station Descent of fetal head (in cm) Effacement Thinning of cervix (in %)
Descent of fetal head: Station Floating Engaged At outlet/crowning
Initial physical assessment & history Admission--rapport Fetal & UC monitoring Vaginal exams, q 2 hours Vital signs Temperature q 4 hours-intact or q 2 hours ROM Educate regarding labor Encourage comfort, position changes, bladder emptying Assess pain, pain tolerance, preferred type of labor/delivery Reassure regarding what is normal, reduceanxiety Care of Laboring PatientEarly Labor • Couple excited, talkative, pain is manageable
Care of Laboring PatientActive Labor • Transition (7-10 cm): Yikes! “out of control”, shaking, nausea/vomiting, sweating, pain is intense • Prepare for delivery • Second stage (Pushing): • Educate/instruct regarding pushing • Assess urge to push and fetal descent • Encourage/motivate patient, assess fatigue • Monitor fetal/maternal response to pushing bulge, crowning • Signs of imminent birth: perineal bulging • Couple quieter, discouraged, pain increasing
Stages of Labor:Second Stage • Pushing & descent of baby (STATION) • Full dilatation (10 cm) to birth • Important NOT to push until full dilation • Assessment: Urge to push? Rectal pressure? • Push only with UC’s • Crowning: baby’s head is visible at the opening of vagina • Cardinal movements of labor youtube.com/watch?v=Xath6kOf0NE&feature=related youtube.com/watch?v=duPxBXN4qMg&feature=related
Mechanisms of labor. A, B, Descent. C, Internal rotation. D, Extension. E, External rotation.
Crowning Crowning In the hospital Alternative settings
Stages of Labor: Third Stage • Placental stage: from birth to delivery of placenta • Placental separation from uterine wall (rise of fundus, sudden gush of blood, lengthening of umbilical cord) • Entire lining of uterus shed • Expulsion of placenta • Normal blood loss: 300-500 mL • If placenta does not deliver spontaneously, can be delivered manually • Pitocin infusion started immediately post delivery of placenta
Critical Thinking • A client is admitted to the labor unit with contractions 2 to 3 minutes apart and lasting 60 to 90 seconds. The client is apprehensive and vomiting. This nurse understands this information to indicate that the client is most likely in what phase of labor? • A) Active • B) Transition • C) Latent • D) Second
Initial Intrapartum AssessmentPages 608-612 • Vital signs • Fetal heart rate pattern, fetal distress • Contraction pattern, intensity, pain • Membrane status--intact, ruptured, nitrizine test, amniotic fluid: clear, meconium, foul odor • Prenatal records, history of pregnancy, complications, previous pregnancies and deliveries, maternal health problems • Psychosocial/family/cultural issues • Labs: CBC, dip urine for protein, glucose, ketones • Vaginal Exam--effacement/dilation/station, fetal presentation/lie. Assesses LABOR PROGRESS
Intrauterine Fetal Resuscitation • *Stop pitocin • Reposition to left lateral, Trendelenberg if needed • Oxygen via mask at 8-10 L/min • Increase IV fluids • SQ terbutaline (0.25 mg) if uterus not relaxing • Vaginal exam for possible cause: prolapse, fetal descent, rupture, abruption • Amnioinfusion for variable decels • Notify MD/midwife
Which strip shows signs that Immediate intervention is needed? Why? What would you do? B A
Experiences of Pain • Etiology • Physiology • Perception • Factors influencing Anxiety Psychological factors Expectations Cultural factors SupportFetal position
Comfort and Pain Relief • Support from doula or coach • Alternative therapies • Relaxation/massage • Focusing and imagery • Breathing • Herbal preparations/aromatherapy • Hypnosis
Comfort and Pain Relief • Pharmacological Measures • Narcotic analgesics • Nubain/Stadol/Demerol (pg. 689) • Regional nerve blocks • Epidural/spinal • Local anesthetic blocks • Pudendal/perineal
Systemic AnalgesiaTable 25-3, pg 690 • Pre-medication Assessment: • Pain level, VS, allergies, drug dependence (withdrawal), vaginal exam/progress in labor, UC pattern, fetal heart rate tracing • Post-medication Assessment: • VS, esp. RR, LOC, dizziness (bedpan), sedation, FHR • Reversal agent: Naloxone (Narcan) • Competes with narcotic for opiate receptors. Used in both mom and baby. (avoid with narcotic dependence)
Regional Anesthesia • Injection of local anesthesia to block specific nerve pathways • Epidural/spinal anesthesia • Systemic toxicity: cardiovascular collapse • Side effects: Hypotension (preload with IV fluids), fetal distress on FHR tracing, spinal HA • Contradindications: coagulation disorders, low platelet count (< 100), allergy, neurologic disease, aspirin use • Nursing care: Preload IV fluids (LR), monitor BP, HR, anesthesia level, FHR, foley cath, maternal positioning
Medication for Pain Relief: Birth • Local anesthesia • Pudendal nerve block (2nd stage, episiotomy, repair) • Local infiltration in perineum (episiotomy, repair) • General anesthesia • Regional contraindicated/emergency • Preparation: hip wedge, preoxygenation, cricoid pressure for intubation • Complications: fetal depression, aspiration of vomitus (Bicitra)
Childbirth at Risk(Ch. 26) Complications of Labor or Delivery
Critical Thinking The client in active labor is requesting pain relief. The physician orders epidural anesthesia for the client. Which of the following parameters should the nurse be prepared to assess immediately after administration of the epidural? • A) For headache. • B) For urinary retention. • C) The blood pressure. • D) The maternal pulse rate.
Precipitous Labor &Birth • Labor in < 3 hours • Risk factors: • Multiparity, oxytocin or amniotomy, hx of precipitate labor • Risks for injury • Maternal: cervical, vaginal & perineal lacerations with possible hemorrhage, pain, anxiety • Fetal: Birth trauma (intracranial bleed, brachial palsy), meconium-stained fluid, fetal distress • Management: close monitoring for cervical changes, induction
Postterm Pregnancy • > 42 weeks • Maternal risks: trauma/hemorrhage due to larger baby, ↑operative delivery/c-section • Fetal risks: placental changes that ↓oxygenation to baby and ↑mortality rate, oligohydramnios (↑cord compression during labor), LGA baby (↑birth trauma, shoulder dystocia), meconium aspiration • Management: > 40 wks, NST, BPP or modified BPP (NST & AFI), induction
Malpresentations • Occiput-posterior (OP) • Prolonged labor, back labor (sacral nerve compression), arrested dilatation/ descent, perineal tears • Usually vaginal, but may need C-Section if baby doesn’t rotate • Management: positioning (side-lying, knee-chest or hand-knees), sacral pressure during UC’s • Transverse Lie • Associated with: pendulous abdomen, uterine masses/fibroids, congenital abnormalities of uterus, hydramnios • Attempt External Cephalic Version, if unsuccessful obligatory C-section
Malpresentations (cont) • Breech presentation Assessment: FHT heard high on the abdomen, Leopold’s, vaginal exam & US. • Higher risk of anoxia from prolapsed cord, traumatic injury to the after coming head, fracture of spine or arm, dysfunctional labor • Usually delivered by C-section
External Version • External cephalic version (37-38 wks): abdominal manipulation to change fetal presentation • Contraindications: multiple gestation, fetal breech is engaged in pelvis, oligohydramnios, nonreactive NST, nuchal cord, vaginal bleeding, IUGR, ROM. • Risks: immediate cesarean birth • Nursing actions: NPO 8 hrs, NST, IV line, terbutaline, continuous FHR, US used to guide manipulations, assess for: labor, fetal distress. O- moms need Rhogam following the procedure
Macrosomia/Shoulder Dystocia • Wt. > 4500 gms (9-10 lbs) • Associated with: • DM, Gestational DM, Multiparity, Postdates, obesity • Risks: • Shoulder dystocia, difficulty delivering the shoulders after head is delivered (obstetrical emergency) • Maternal: vaginal/cervical tears, pp hemorrhage, rupture • Fetal: compressed cord, fractured clavical, asphyxia & neurologic damage, brachial plexus injury (Erb’sPalsy) • S/S: Turtle sign • Nursing interventions: McRoberts maneuvers, suprapubic pressure. PP: assess for uterine atony/hemorrhage; trauma, cerebral or neurologic damage to baby
Multiple Gestation • Monozygotic (identical) twins: can have 1 or 2 placentas, chorions, or amnions (↑risk if all shared) • Dizygotic (fraternal) twins: 2 of everything. • Dx: faster than usual growth of uterus, ↑AFP, HCG, Ultrasound • Risks: • Maternal: SAB, gestational DM, HTN/preeclampsia/HELLP, hydramnios, PT labor & delivery • Fetal: Preterm birth, twin-to-twin transfusion
Multiple Gestation (cont) • Management: • US to determine what type of twins • Prevention of PT labor/routine cervical measurements (US) • NST surveillance • Birth: depends on maternal & fetal complications and fetal position/ presentation • Examination of placenta • Close monitoring PP for hemorrhage (atony)