Download
1 / 21
260 likes | 580 Views
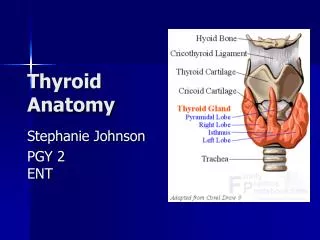
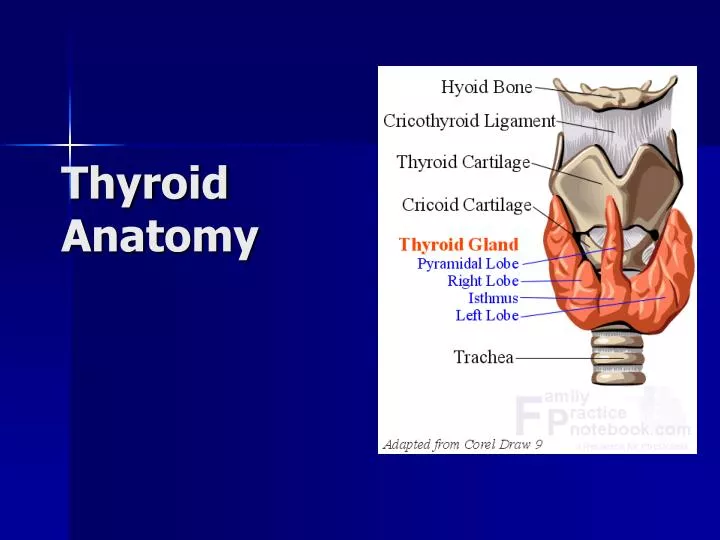
Thyroid Anatomy. Background. What: brownish-red, highly vascular gland Location: ant neck at C5-T1, overlays 2 nd – 4 th tracheal rings Avg width: 12-15 mm (each lobe) Avg height: 50-60 mm long Avg weight: 25-30 g in adults (slightly more in women)

E N D
Background • What: brownish-red, highly vascular gland • Location: ant neck at C5-T1, overlays 2nd – 4th tracheal rings • Avg width: 12-15 mm (each lobe) • Avg height: 50-60 mm long • Avg weight: 25-30 g in adults (slightly more in women) **enlarges during menstruation and pregnancy**
Background Pyramidal lobe: • often ascends from the isthmus or the adjacent part of either lobe (usu L) up to the hyoid bone • may be attached by a fibrous/fibromuscular band “levator” of the thyroid gland
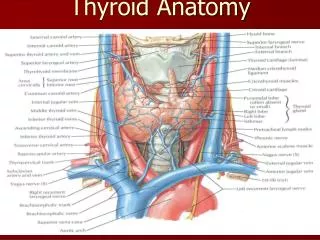
Transverse view: relationship to other NB structures in neck
Structure • Under middle layer of deep cervical fascia (pretracheal) thyroid inner true capsule thin and closely adherent to the gland • capsule extensions within the gland form septae, dividing it into lobes and lobules • lobules are composed of follicles = structural units of the gland layer epithelium enclosing a colloid-filled cavity • colloid (pink on H&E stain) contains an iodinated glycoprotein, iodothyroglobulin (precursor of thyroid hormones).
Structure • Follicles = variable size • surrounded by dense plexuses of fenestrated capillaries, lymphatic vessels, and sympathetic nerves.
Structure Epithelial cells = 2 types: • principal (ie: follicular) – formation of colloid (iodothyroglobulin) • parafollicular (ie: C cells -clear, light), lie adjacent to follicles w/in basal lamina produce calcitonin
Relation w/ Strap muscles • Lateral - sternothyroid • Anterior • omohyoid muscle • sternohyoid • Inferior - SCM (lower portion) ** careful - motor nerve supply from the ansa cervicalis enters these muscles inferiorly.
Recurrent laryngeal nerve • Recall: innervates all larynx except cricothyroid • Closely assoc with ITA (see next slides for details) • NB: ‘non recurrent LN’ ~5/1000 pt’s on R side • When retroesophageal R SCA from dorsal aortic arch • NRLN - branches fr X at ~ cricoid cartilage • directly enters the larynx without looping around SC • L sided - only when R aortic arch and ligamentum arteriosum concurrent w/ L retroesophageal subclavian artery.
Vascular Anatomy ARTERIAL: • superior and inferior thyroid arteries (occ thyroidea ima) • ++ collateral anastomoses (ipsi and contralaterally) • thyroid ima (when pres) originates from aortic arch or innominate artery, enters the thyroid at inferior border of isthmus.
Vascular Anatomy SUPERIOR THYROID ARTERY • first anterior branch ECA • descends laterally to the larynx under the omohyoid and sternohyoid muscles • runs superficially on the anterior border of the lateral lobe, sending a branch deep into the gland before curving toward the isthmus where it anastomoses with the contralateral artery
Vascular anatomy SUPERIOR THYROID ARTERY: Relationship with SLN: • Cephalad to the superior pole, ext branch of SLN runs w/ STA before turning medially supply cricothyroid muscle **careful when ligating artery**
Vascular anatomy INFERIOR THYROID ARTERY SCA thyrocervical trunk ITA • ITA ascends vertically and then curves medially to enter the tracheoesophageal groove (posterior to carotid sheath) • Branches penetrate the posterior aspect of the lateral lobe
Vascular anatomy Relationship with RLN: • RLN ascends in the TE groove and enters the larynx b/w the inferior cornu of the thyroid cartilage and the arch of the cricoid • RLN can be found after it emerges from the superior thoracic outlet: • Sup: thyroid lobe • Lat: common carotid artery • Medial: trachea
Vascular anatomy **Careful - relationship between RLN and ITA highly variable (Redd, 1943 – described 28 variations) Examples: • Deep to ITA (40%) • superficial (20%) • b/w branches of the artery (35%) **also – only 17% of the time is the nerve/artery relationship the same on both sides **at level ITA – extralaryngeal branches RLN present 5% of the time
Vascular anatomy VENOUS: 3 pairs of veins: • STV – asc along STA and becomes a tributary of the IJV • MTV – directly lateral IJV • ITV (variable): • R – passes ant to innominate a R BCV or ant trachea L BCV • L – drainage L BCV **occ – both inf veins form a common trunk “thyroid ima vein” empties into L BCV
Lymphatics • Extensive, multidirectional flow • periglandular prelaryngeal (Delphian) pretracheal paratracheal (along RLN) brachiocephalic (sup mediastinum) deep cervical thoracic duct • NB: regional mets of thyroid carcinoma are superior and lateral, along IJV ie: invasion of the pretracheal and paratracheal LNs and obstruction of normal lymph flow.
Innervation Principally from ANS • Parasympathetic fibers – from vagus • Sympathetic fibers – from superior, middle, and inferior ganglia of the sympathetic trunk Enter the gland along with the blood vessels.
References: • Schwartz • www.emedicine.com • www.utdol.com • Gray’s anatomy • http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=endocrin.box.330 • Netter’s anatomy