Download
1 / 25
250 likes | 369 Views
Pain Staffing Survey for Academic Practices. Society of Academic Anesthesia Chairs Association of Academic Program Directors November 5, 2004. Loyola University Medical Center. All Anesthesiology Department chairs are faced with the operational conundrums of their pain clinics.

E N D
Pain Staffing Survey for Academic Practices Society of Academic Anesthesia Chairs Association of Academic Program Directors November 5, 2004 Loyola University Medical Center
All Anesthesiology Department chairs are faced with the operational conundrums of their pain clinics.
Part procedural, part clinic based, these programs can be problematic since faculty are hard to recruit and retain. In addition, ancillary staff can consume a huge amount of monetary resources and clinic space may be difficult to acquire. Part procedural, part clinic based, these programs can be problematic since faculty are hard to recruit and retain. In addition, ancillary staff can consume a huge amount of monetary resources and clinic space may be difficult to acquire.
Each anesthesiology department pain group and staffing model may be unique. The adage “when you see one pain program, you’ve seen one pain program” may apply.
This survey attempts to gather information on patient volumes, procedural activity, staffing, funding and coverage sites to determine a common model, if any, for academic pain programs across the country.
A total of 48 programs or 36% of the membership responded to this survey with most areas of the country represented.
Patient Volumes E&M VisitsProceduresAPS 3,959 2,388 3,650 504 – 8,590 800 – 24,469 830 – 14,000 Represented as median values with ranges
Patient Volumes Interventional Conscious Average Pain Procedures SedationLength Mins. 150 538 45 9 – 5,065 16 – 4,800 20 – 60 Represented as median values with ranges
Staffing for Pain Clinic Total Staff Full Time in ClinicsStaff 4.5 3.2 0 – 21
Staffing for Pain Clinic PhysiciansFellowsResidentsRN’s 3.0 3.0 1.0 2 1 – 15 0 – 7 0 - 3 0 - 7 Represented as median values with ranges
Ancillary Staff Patient Care Techs 3 programs Physician Asst. 4 programs Nurse Asst. 4 programs Medical Asst. 3 programs Radiology/Fluoroscopy 4 programs
Acute Pain Service Staffing PhysiciansFellowsResidentsRN’s 1.1 1 0.5 1 0 – 7 0 – 5 0 - 3 0 - 4 Represented as median values with ranges
Other Personnel Physician Asst. 1 program Nurse Asst. 1 program Medical Asst. 1 program
Funding for Pain Service Hospital Support (%) Physician 14 Clinic Staff 55 APS Staff 32
Funding for Pain Service Dept. Support (%) Physician 82 Clinic Staff 59 APS Staff 59
Salary Model for Pain Staff Based on SAAC/AAPD Survey 38% Salary with incentives based on number of RVU’s over baseline 33% Combination of both 8% Total production benchmarked on professional activities 8% No response 13%
If hospital funded, what benchmark is used to staff RN’s in clinic: • Number of E&M visits • One RN / FTE physician adjusted by productivity • Staff to workload time/task analysis • Staff to number of procedures and visits
Pain physician provides coverage in operating room Yes – 50% No – 50% All staff may provide operating room coverage or as little as one out of group may provide coverage
Private group affiliation with pain faculty? Yes – 25% No – 71%
Does a private pain group participate in fellowship training? Yes – 29% No – 58%
Does your academic pain group receive a high number of referrals for chronic pain patients on high dose opioid therapy? Yes – 83% No – 17%
Does your Pain Program have a multidisciplinary addiction center for detoxification of pain patients? Yes – 8% No – 92%
Multidisciplinary Pain Program Composition • Psychiatry • Family Medicine • Rehab Medicine (PMER) • Neurology • Neurosurgery
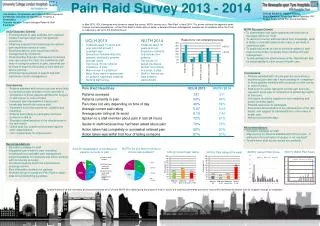
Findings • Most pain clinics staff with full time physicians, fellows, residents, and RN’s • Funding for physicians comes primarily from departmental support while 50% of pain department clinical staff are supported by anesthesiology department, half are supported by the hospital • Salaries are based either on standard formats for academic faculty or salary plus incentives based on RVU’s • Pain physicians provide OR support in 50% of programs while 50% work exclusively in pain related clinical activity • 25% of program have affiliations with private pain groups • Only a few programs have multidisciplinary pain programs