Download
1 / 30
350 likes | 519 Views
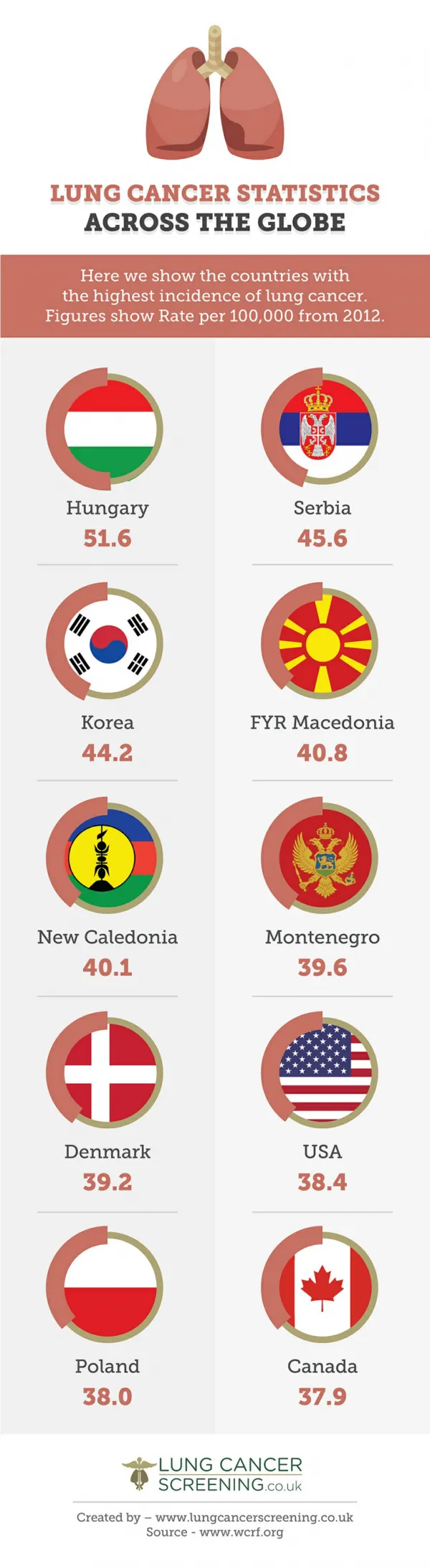
Clinical Application of Next Generation Sequencing for Personalized Medicine in Solid Tumors Presented by: Ryan Bender, PhD FACMG. Cancer Statistics. Evolution of Knowledge in NSCLC. Traditionally, non-small-cell lung cancers have been classified according to histological features.

E N D
Clinical Application of Next Generation Sequencing for Personalized Medicine in Solid TumorsPresented by: Ryan Bender, PhD FACMG
Evolution of Knowledge in NSCLC • Traditionally, non-small-cell lung cancers have been classified according to histological features. • Various driver mutations have been associated with these cancers over time. • The mutations are mutually exclusive, except for those in PIK3CA. • Mutations associated with drug sensitivityEGFR Gly719X, exon 19 deletion, Leu858Arg, Leu861Gln • Mutations associated with primary drug resistanceEGFR exon 20 insertions • Mutations associated with acquired drug resistanceEGFR Thr790Met, Asp761Tyr, Leu747Ser, Thr854Ala New driver mutations in non-small-cell lung cancer William Pao, Nicolas Girard, Lancet Oncol 2011; 12: 175–80
Next-Generation Sequencing Greater volume of clinically-actionable information • Additional markers analyzed • Pathways more fully interrogated • Clinical trials opportunities expanded Additional service and reporting options • Expanded NGS panel for Select and Comprehensive profiles • 45 gene pan-tumor NGS panel Enhanced specimen-friendly requirements • Smaller specimens accepted (8-10 unstained, unbaked, positively charged slides) • FFPEor Formalin samples accepted
IlluminaMiSeqTruSeqAmplicon Cancer Hotspot Panel Validation • Used 80 FFPE samples (70 FFPE tissue samples, 6 cell lines and 4 HapMap samples) • >98% accuracy when compared to Sanger. • One discordant result stemming from misalignment of A502_Y503dup mutation in KIT (Using Pindel and validating bioinformatics solution) • >97% precision for inter-operator, inter-lot and inter-machine tests (Most sources of discordance involved indeterminate results) • Linear and reliable variant detection down to 5% • All reported mutations have >99% confidence at a sensitivity of 10%
Anti-EGFR Monoclonal Antibodies • Cetuximab (Erbitux) • Manufactured and marketed by ImClone and Bristol-Myers Squibb (~$30,000/ 8 week cycle) • Approved in 2006 for treatment of squamous cell carcinomas of the head and neck • Panitumamab (Vectibix) • Manufactured by Amgen (~$100,000/year) • Approved for treatment of colorectal cancer in 2006 • 2009 – Discovered KRAS mutations are negative indicators of response to EGFR mabs in colorectal cancer
Benefit of Molecular Profiling on Therapy Response Adapted from DeRooke et al. 2010
Roche cobas BRAF Mutation Assay • FDA approved companion diagnostic for Zelboraf use • Specific to the p.V600E mutation • Can pick up other mutations – p.V600K, p.V600D, p.V600E(2), V600_K601delinsD • Does not detect p.V600R
BRAF Mutation Analysis • Sequencing • V600E • Other V600 mutations • Exon 15 insertions/deletions (V600_K601delinsE/D) • L597 and K601 mutations • Exon 11 mutations • FDA Approved Method – BRAF cobas 4800 V600 mutation test • PCR based • FDA approved companion diagnostic for Zelboraf and Debrafenib
Case #1 • 64 y/o patient presenting with growth on spinal cord • Biopsy reveal heavily pigmented nodule positive for MART-1, HMB-45 and MITF • Malignant melanoma with unknown primary favored as Dx • Sample tested for standard melanoma markers • NGS performed with a request to report BRAF and KIT mutation status • GNA11 Q209L mutation detected
Conclusions • NGS sequencing is a high throughput method for interrogation of the mutation status of a large number of biomarkers • Pathway analysis is expensive and laborious by previous methods – becoming standard of care for cancer therapy • NGS adds additional information that some companion diagnostics do not provide • Potential benefit of incidental findings to clarify diagnosis or detect rare finding