Download
1 / 44
500 likes | 1.26k Views
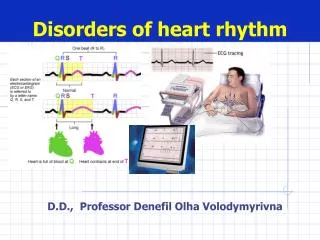
Disorder of heart rhythm. Ph.D. , MD , Assistant Professor Potikha N.Ya. ETIOLOGY. Functional violations and influences ANS activity changes Physical load Body’s t 0 change ( fever ; hyperthermia , hypothermia ) Hormone’s blood concentration changes Intracranial pressure increase

E N D
Disorder of heart rhythm Ph.D., MD,Assistant ProfessorPotikha N.Ya
ETIOLOGY Functionalviolations and influences • ANS activity changes • Physical load • Body’st0change(fever; hyperthermia, hypothermia) • Hormone’s blood concentration changes • Intracranial pressure increase • Infection(flu, typhoid) • breathing(in children)
ETIOLOGY Organicfactors • inflammation of myocardium (infection, uninfection) • myocardium dystrophy (hypoxia, ischemia, amiloidosis) • myocardium necrosis
ETIOLOGY • Toxic influences - alcohol • medicines (beta-adrenoblockers) • catecholamines • glucocorticoids • bacterial toxins • phosphororganic substances
ETIOLOGY • Hormone balance violation • Hyperthyroidism • Hypothyroidism • suprarenal glandshyperfunction • suprarenal glands hypofunction
ETIOLOGY • Ions imbalance • changesofK, Na, Ca, Mg, Cl cardiomyocytes concentration (because long time using diuretics, uncontrolledusing mineral water) Organism more sensitive to К+deficit than to АТP one
ETIOLOGY • Mechanical influences • catheter using (for diagnosis and for treatment) • operation • chest trauma
PATHOGENESIS(pathological condition of the heart) • Injury of conductive system differentparts • No electrical homogenous of myocardium • No electricalfunctionalstableof myocardium(violation of MRP)
PATHOGENESIS(ARRHYTHMIAS THEORIES) Electricity of injury (No electrical homogenous of myocardium) Zone of injuryNormal tissue membrane is partlydepolarized membrane is completely depolarized (MRP = 0 mV or +20 mV) (MRP = -90 mV) potential difference appearsbetween both these zones and ectopic driveractivates
PATHOGENESIS(ARRHYTHMIAS THEORIES) Ectopic rhythm driver activation (electricalfunctionalunstable myocardium ) Subthreshold oscillations : unstable MRP causeslow amplitude fluctuation, which can causeearly depolarization(hypoxia, K+ deficit, heart distention)
PATHOGENESIS(ARRHYTHMIAS THEORIES) Ectopic rhythm driver activation (electricalfunctionalunstable myocardium ) Overthreshold oscillations :appears at retardation or at breakingof repolarization (MAP cann’t be transformed in to MRP and new action potentialarrears and as a result - ectopic rhythm)
PATHOGENESIS(ARRHYTHMIAS THEORIES) “Re-entry” Gist:repeat or multiple impulses enter in some area of conductive system of the heart or in contractile myocardium Condition: • There are 2 conductive ways, which are separated functionally or structurally • There is block of impulses transmission thought the oneconductive way • Impulses transmission is possible only in reverse route
ARRHYTHMIAS CLASSIFICATION • Automatism violations • Conduction violations • Combined violations (automatism, conduction and excitability)
Automatism violation *Nomotopic(gist – violation of impulsesformation in sinus node) 1. Sinus tachycardia 2. Sinus bradycardia 3. Sinus arrhythmia (respiratory) *Heterotopic rhythms(gist – dominance of ectopic area activity) 1. Tardy ectopic rhythm (vicarious, passive) 2. Unparoxismal tachycardia 3. Migration of supraventricular rhythm driver
NomotopicAutomatism violationSinus tachycardia Reasons: physicalload, emotional stress, heart failure, myocardium ischemia or infarction, myocardium dystrophy ECG: sinus rhythm, HR90-180/min, R-R duration<0,60 c
NomotopicAutomatism violationSinus bradycardia Reasons: n. Vagus high activity (sportsmen, flu, typhoid),intracranial pressure increase (results from irritation of n.Vagus nucleas) ECG: sinus rhythm, HR59-40/min, R-R duration>1,0 с sec sec
NomotopicAutomatism violationSinus (respiratory) arrhythmia Reasons: breathing (in children), after grip, neurocirculative dystone ECG:sinus rhythm, difference between the shortest R-R and longestR-R >0,15 sec s s s s
Heterotopic rhythmsTardy ectopic rhythm (vicarious, passive) Source:atrium, AV node, ventricle Meaning:protection of the heart at long time asystole (at SA node arrest) Kinds: -atrial -аtrial-ventricular • Ventricular (HR <40/min)
Heterotopic rhythmsUnparoxismal tachycardia Source: atrium, AV node , ventricle ECG: -HR90-130/min - progressive beginning and finishing - regular ventriclerhythm
Heterotopic rhythmsMigration of supraventricular rhythm driver Gradual removal of rhythm driver from SA node to AV node ECG: P wave configurationviolation Change ofP-Q duration Arrhythmia
heart block Sinus atrial (or SA node arrest) - Atrial - Atrial-ventricular -ventricular pre-excitation syndrome 1. WPW syndrome 2. CLC syndrome Conduction violations
Conduction violations Sinus atrial block (arrest) Violation of impulses transmission fromSA-node to atriums (most often - noncomplete) ECG:PQRST complex is absent compensatory pause is equal 2 (R-R) Some time 3-4PQRST complexes fall out and tardy ectopic rhythm (vicarious, passive) appears
Conduction violations Atrial block Violation of impulses transmission through the atrium conductive system ECG:Рduration>0,11 sec, Р -deformed
Conduction violations АV-block Violation of impulses transmission through the AV node 1 degree 2 degree: Mobitz type I, Mobitz type II, type III(high degree AV block) 3 degree(complete AV block)
Conduction violations АV-block 1 degree ECG: PQ>0,2 sec
Conduction violations АV-block 2 degree *Mobitz type I (Venkebah) - Progressive increase ofPQ duration (Venkebah’s pariods)with after fall out QRST *Mobitz type II - PQare prolonged orNbut their length is constant QRSTfall out (periodicity is 2:1, some time 3:1, 4:1) * type III(high degree AV block) - QRSTfall out (periodicity is 2:1, 3:1, 4:1) bradycardia (tardy ectopic rhythm arrears) Symptoms: dizziness, unconsciousness
Conduction violations АV-block 3 degree (complete) * Absolute stop impulses conduction from atriums to ventricles * Independent excitation and contraction of the atriums and ventricles ECG: Рamount > QRS amount, P waves and QRS complexes appearindependently, some time Р are masked byQRS orT and that causes their deformation
Conduction violations АV block Stokes-Adams’s syndrome Reasons: - long timeasystole(more than 10-20 seс) (occures at transition ofАV-block 2 degreetype IIIinto complete АV-block - long timeasystoleat АV-block3degree(complete) - long timeasystoleat ventricles fibrillation because АV-block3 degree Signs: unconsciousness, convulsions (because: decreased heart output and brain hypoxia) Prognosis:at every attack patient can die
Conduction violations ventricleblock • Violation of impulses conduction in ventricle conductivesystem Giss’sbundle branches block * blockof 1 branche * blockof 2 branches * blockof 3 branches * local intraventricleblock ECG:QRSdeformation
Conduction violations Pre-excitation syndrome WPW (Wolff-Parkinson-White) syndrome Reason: additional Kent’s bungle (impulses don’t travel through the AV node but through Kent’s brunch) ECG: PQ<0,12 sec, QRS is deformed and wide because Δ-wave, ST и T arelocalesed dyscordly, pre-excitation of the ventricles wave
Conduction violations Pre-excitation syndrome CLC (Clerk-Levy-Critesco) syndrome (syndrome of shortPQ) Reason: additional Jaims’s bungle(impulses came to ventricles earlier than through the AV node) ECG: PQ<0,12 sec, QRSunchanged
Conduction violations Pre-excitation syndrome Complications Pre-excitationofanyarea in ventricle Y Formation of electricalunstable myocardium Y “Re-entry”mechanism activation Y Ectopic driver appearens Y extrasistole paroxysmal tachycardia ventricle flutter (ventricular tachycardia)
Arrhythmias in the result of combined violations (automatism, conduction and excitability) • Extrasistole • Paroxysmal tachycardia • Atrium flutter • Atrium fibrillation • Ventricle flutter (ventricular tachycardia) • Ventricle fibrillation
Extrasistole extraordinary systole in the result of ectopic pacemaker activation Reason: * Membrane’shigh oscillative activity * “re-entry” mechanism Types, ECGsigns: - atrial(Р deformed) - atrial-ventricular(Р appears afterQRS) - ventricular(no Р before QRS, QRS deformation, complete compensatory pouse)
Extrasistole(atrial) ECGsigns: Р deformation
Extrasistole(AV) ECGsigns:Р appears afterQRS
Extrasistole(ventricular) ECGsigns:no Р before QRS, deformation ofQRS, complete compensatory pause
Paroxysmal tachycardia Attack of the heart contractions (140-250/min),which sudden onset and offsetat regular rhythm Mechanisms:- “re-entry”, ectopic driver activation Types, ECGsigns : - atrial (Р deformed) - atrial-ventricular (Р appears afterQRS) - ventricular(no Р before QRS, QRS is deformed and wide) Duration – from some seconds to some minutes
Atrium flutter rapid and regular atrial contructions with a rate from 240 to 450/min Mechanisms: re-entry, ectopic driver activation ECG: regular and rapid F-waves (sawtooth pattern), QRSunchanged
Atrium fibrillation rapid and unregular atrial contructions with frequency 350-700/min Mechanisms: re-entry, ectopic driver activation ECG:unregular and rapid f-waves (sawtooth pattern), complexes QRS appear irregular
Ventricle flutter and fibrillationfibrillation Flutter – frequent (200-300/min) regularexcitation and contraction of the ventricles because impulses from ectopic driver circulates constantly (“re-entry”) ECG:no P, QRS is wide Fibrillation – frequent (200-500/min),inregular andhaotic excitation and contraction of cardiomyocyte’s separated groups in ventricles (finally ventricles don’t contract) ECG: changed shape and amplitude of the waves without any intervals