Download
1 / 37
500 likes | 1.01k Views
Homeostatic Control of Metabolism. Food Intake. How does your body know when to eat? How does your body know how much to eat? Two ‘ competing ’ behavioral states: Appetite = desire for food Satiety = sense of fullness. Hypothalamic Centers. Feeding center – tonically active

E N D
Food Intake • How does your body know when to eat? • How does your body know how much to eat? • Two ‘competing’ behavioral states: • Appetite = desire for food • Satiety = sense of fullness
Hypothalamic Centers • Feeding center – tonically active • Satiety center – inhibits feeding center Figure 11-3
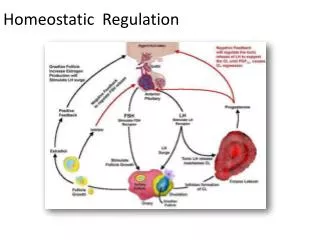
Regulation: Classic Theories • Glucostatic theory: glucose levels control the feeding and satiety centers in hypothalamus • Low [glucose] – satiety center suppressed • High [glucose] – satiety center inhibits feeding center • Lipostatic theory: body fat stores regulate the feeding and satiety centers • Low fat levels increased eating • Recent discovery of leptin and neuropeptide Y provides support
Peptides Regulate Feeding • Input to hypothalamus: • Neural from cerebral cortex • Neural from limbic system • Peptide hormones from GI tract • Adipocytokines from adipose tissue
Peptides Regulate Feeding Note the diversity of peptide origins! cholecystokinin =
Peptides Regulate Feeding inhibition Figure 22-1
We Eat To Do Work • Energy input = energy output • Energy output = work + heat • 3 categories of work: • Transport work – moving molecules from one side of membrane to the other • Mechanical work – movement • Chemical work – synthesis and storage of molecules • Short-term energy storage – ATP • Long-term energy storage – glycogen, fat
Metabolism = sum of all chemical reactions in the body • Anabolic pathways – synthesize large molecules from smaller • Catabolic pathways – break large molecules into smaller
Metabolism • Divided into two states: • Fed (or Absorptive) state • After a meal • Anabolic – energy is stored • Fasted (or Post-absorptive) state • Molecules from meal no longer in bloodstream • Catabolic – storage molecules broken down
Fate of Ingested Molecules • Immediate use in energy production: nutrient pools • Synthesis into needed molecules (growth, maintenance) • Storage for later use • Fate depends on type of molecule: carbohydrate, protein, or fat
DIET Fats Carbohydrates Proteins Build proteins Free fatty acids + glycerol Excess stored Proteinsynthesis Glycogenesis Aminoacids Excess stored Glucose Fatstores Lipogenesis Excess glucose Lipogenesis Bodyprotein Glycogenstores Urine Lipolysis Glycogenolysis Glucose pool Gluconeogenesis Free fattyacid pool Range of normalplasma glucose Amino acidpool Many immediately used Excess converted in liver Many immediately used Metabolism inmost tissues Brainmetabolism Excess nutrients Figure 22-2
What Controls This? • Hormones control metabolism by altering enzyme activity and molecule movement • Push-pull control: different enzymes catalyze forward and reverse reactions
Push-Pull Control INSULIN enzyme 1 enhanced, enzyme 2 inhibited enzyme 1 inhibited, enzyme 2 enhanced GLUCAGON Figure 22-4
Metabolism is Controlled by Ratio of Insulin and Glucagon Anabolic Catabolic Figure 22-9
Fed State Many immediately used
Fasted State 1 2 Liver glycogenbecomes glucose. Adipose lipidsbecome freefatty acids andglycerol thatenter blood. Triglyceride stores Free fattyacids Liverglycogenstores Free fattyacids Glycerol -oxidation Glycogenolysis Gluconeogenesis Energyproduction Ketonebodies Energy production Glucose Glycogen Proteins Gluconeogenesis Pyruvate or Lactate Aminoacids Ketonebodies Glucose Energy production 3 Muscle glycogen can be used for energy.Muscles also use fatty acids and breakdown their proteins to amino acids thatenter the blood. 4 Brain can useonly glucose andketones for energy. Figure 22-7
Pancreas – Islets of Langerhans Figure 22-8
Insulin • Origin in β cells of pancreas • Peptide hormone • Transported dissolved in plasma • Half-life ~5 min • Target tissues: liver, muscle, adipose tissue
Insulin • Secretion promoted by: • High plasma [glucose] (> 100 mg/dL) • Increased plasma amino acids • Feedforward effects of GI hormones • Glucagon-like peptide-1 (GLP-1) • Gastric inhibitory peptide (GIP) • Anticipatory release of insulin • Parasympathetic input to β cells • Secretion inhibited by: • Sympathetic input • Reduced plasma [glucose]
Insulin Mechanism of Action Extracellularfluid 1 Insulin binds to tyrosinekinase receptor. Insulin 1 2 Receptor phosphorylatesinsulin-receptor substrates (IRS). 3 Second messenger pathwaysalter protein synthesis andexisting proteins. GLUT4 2 IRS IRS P Transportactivity 4 3 4 Membrane transportis modified. Secondmessengerpathways Nucleus Enzymes or 5 Cell metabolism ischanged. 5 Transcriptionfactors Changes inmetabolism Figure 22-11
Insulin Lowers Plasma Glucose • Increases glucose transport into most insulin-sensitive cells • Enhances cellular utilization and storage of glucose • Enhances utilization of amino acids • Promotes fat synthesis
Insulin Increases Glucose Transport • Required for resting skeletal muscle and adipose tissue • Moves GLUT-4 transporters to cell membrane • Exercising skeletal muscle does not require insulin for glucose uptake • In liver cells, indirect influence on glucose transport
Insulin Increases Glucose Transport:Skeletal Muscle & Adipose Tissue GLUT-4 transporters moved to cell membrane Figure 22-12
Insulin Increases Glucose Transport:Indirect in Liver Cells Insulin activates hexokinase, keeps IC [glucose] low Figure 22-13
Insulin Enhances Utilization and Storage of Glucose • Activates enzymes for: • Glycolysis – glucose utilization • Glycogenesis – glycogen synthesis • Lipogenesis – fat synthesis • Inhibits enzymes for: • Glycogenolysis – glycogen breakdown • Gluconeogenesis – glucose synthesis
Insulin Enhances Utilization of Amino Acids • Activates enzymes for protein synthesis in liver and muscle • Inhibits enzymes that promote protein breakdown (no gluconeogenesis) • Excess amino acids converted into fatty acids
Insulin Promotes Fat Synthesis • Inhibits β-oxidation of fatty acids • Promotes conversion of excess glucose into triglycerides • Excess triglycerides stored in adipose tissue
Energy storage Glucose metabolism Figure 22-14
Glucagon • Origin in α cells of pancreas • Peptide hormone • Transported dissolved in plasma • Half-life ~5 min • Target tissues: mostly liver • α cells require insulin to uptake glucose
Glucagon • Secretion promoted by: • Low plasma [glucose] (< 100 mg/dL) • Increased plasma amino acids • Sympathetic input • Secretion inhibited by increased [glucose] • Inhibition by insulin??
Glucagon Raises Plasma Glucose • Main purpose is to respond to hypoglycemia • Activates enzymes for: • Glycogenolysis – glycogen breakdown • Gluconeogenesis – glucose synthesis
Response to Hypoglycemia in Fasted State Figure 22-15
Diabetes Mellitus • Family of diseases • Chronic elevated plasma glucose levels = hyperglycemia • Two types: • Type 1 – insulin deficiency • Type 2 – ‘insulin-resistant’ diabetes; cells do not respond to insulin
Type 1 Diabetes • ~10% of cases • Absorb nutrients normally, but no insulin released – what happens? • Cells shift to fasted state, leading to glucose production! • Results in hyperglycemia and cascading effects
Type 2 Diabetes • ~90% of cases • Target cells do not respond normally to insulin • Delayed response to ingested glucose • Leads to hyperglycemia • Often have elevated glucagon – why? • No uptake of glucose by α cells • Release glucagon • Exercise and modified diet help treat – why?